
Abstract
BACKGROUND AND PURPOSE: Important information regarding fluoroscopically guided lumbar puncture (FGLP) performance and referrals is lacking. The purpose of our study was to elucidate the success rate for initial FGLP attempts and re-attempts, reasons for unsuccessful FGLPs, and the relationship between clinical indications and whether patients will undergo a fluoroscopically guided re-attempt, among others.
MATERIALS AND METHODS: This retrospective study analyzed failed FGLP attempts in hospitalized adult patients at an academic hospital between June 2016 and March 2022. Unsuccessful FGLPs were labeled as insufficient CSF egress. FGLP reports and patients’ clinical charts were analyzed for pertinent information such as clinical indication, reason for failure, whether patients received IV fluid before fluoroscopically guided spinal puncture attempt, and which patients returned for another FGLP attempt. Patients’ ages and sex were analyzed using descriptive statistics. The OR was used to investigate the relationship between the clinical indications to perform FGLP and whether patients returned for a re-attempt.
RESULTS: Sixty-three of 1389 (4.5%) patients (median age, 62 years) had failed the initial FGLPs administered by 39 trainees. Twenty-eight of 63 (44.4%) patients (median age, 64 years) underwent a re-attempt within a median of 2 days after the first attempt, and 27/28 (96.4%) re-attempts were successful. A dry tap, no egress of CSF was the top reason (58.7%) for failed FGLP, and 12/13 of patients had a successful FGLP after IV hydration. Twenty-seven of 63 (43%) patients did not undergo a repeat attempt, and 100% were subsequently discharged from the hospital. There was no difference (P > .05) in the likelihood of patients returning for a repeat FGLP based on the clinical indications.
CONCLUSIONS: Initial and repeat FGLPs have very high success rates. No difference exists in the likelihood of patients returning for a re-attempt based on clinical indication.
ABBREVIATIONS:
- BMI
- body mass index
- FG
- fluoroscopically guided
- FGLP
- fluoroscopically guided lumbar puncture
- LP
- lumbar puncture
Lumbar punctures (LPs) are a commonly performed procedure to obtain CSF. Typically, LPs are performed successfully without imaging guidance, with a reported success rate of ∼72%.1 When unsuccessful, these procedures are performed on adults using image guidance, usually under fluoroscopy in the radiology department. A prior study demonstrated a high success rate in the performance of fluoroscopically guided lumbar punctures (FGLPs), with most of the unsuccessful attempts occurring due to an inability to collect CSF, even though the needle was located in the spinal canal (dry tap).2 Other reasons for unsuccessful FGLP attempts included degenerative changes preventing entry of the LP needle into the spinal canal, and marked obesity precluding proper guidance and visualization and entry into the spinal canal, among others.
A failed FGLP attempt poses potential challenges to patient management, particularly if CSF analysis is crucial to determine appropriate treatment. In addition, failed FGLPs can negatively impact the proper function of the FGLP service because, in our experience, repeat FGLPs will require further analysis regarding the site of entry of the spinal needle (ie, cervical or lumbar) and whether the patient has been hydrated, among others. A properly functioning and efficient FGLP service is particularly important because FGLP referrals continue to increase.3
Prior studies have analyzed the optimization of performing FGLPs,4⇓-6 complications,7,8 training,2,9 and the impact on workflow and residency training,10,11 and many studies have analyzed neuroradiologists’ performance and miss rates for both attendings and trainees regarding the interpretation of diagnostic studies.12,13 However, there is not much information regarding multiple factors related to FGLP performance and referral, potentially helping streamline the process. The purpose of our study was to elucidate the success rate for initial FGLPs and re-attempts, the reasons for unsuccessful FGLPs, and the relationship between clinical indications and whether patients will undergo an FGLP re-attempt, among others.
MATERIALS AND METHODS
The present study was approved by the local institutional review board and is compliant with the Health Insurance Portability and Accountability Act.
Procedure Technique and Operators
Following a written informed consent for the diagnostic LP procedure, all patients underwent FGLP and cervical spinal puncture by means of a C-arm fluoroscopy machine in 1 neurointerventional suite. FGLPs were primarily performed by radiology residents and neuroradiology fellows under the supervision of a neuroradiology attending (range, 7–12 attendings) or independently during nonregular working hours, in a workflow that is similar to that in other academic hospitals;14 attending experience in FGLPs ranged from 1–20+ years. The level of supervision varied among attendings, ranging from directly observing the entire setup and performance of FGLP to being present in a reading room located less than a 20-second walk from the fluoroscopy room and assisting in the procedure as needed.
The range of experience in performing prior FGLPs was large for trainees, varying from the first FGLP attempt (R1s) to having performed >25 FGLPs (R3–R4s and neuroradiology fellows).
Before the FGLP attempt, typically, the lumbar level to access and approach was discussed between the supervising attending and trainee performing the FGLP. We primarily attempt to enter the spinal canal at L2–3 or L3–4 but ultimately leave it to the supervising attending’s discretion, often after the attending has reviewed relevant spinal imaging, if available.
The initial FGLP was typically attempted by the trainee, and if unsuccessful, the supervising attending would attempt it if the patient agreed. All cervical punctures were performed by 1 attending.
Fluoroscopically guided (FG) spinal punctures were performed using techniques as dictated by the American Society of Neuroradiology guidelines and American College of Radiology–American Society of Neuroradiology–Society for Pediatric Radiology parameters with the patient in a prone or lateral position, including the use of local anesthetic15 and iodine and chlorhexidine to clean the skin. The lumbar spinal canal was accessed using the interlaminar or interspinous approach, and the cervical spinal canal was accessed at the level of C1–2 via a lateral approach using a Quincke 22-ga needle. A successful FGLP or cervical spinal puncture involved confirmation of the spinal needle in the spinal canal on fluoroscopy (ideally in the center of the canal, confirmed using anterior-posterior and/or lateral views) and egress of the CSF, enough for collection, after the removal of the stylet.
Patient Population
The patient charts of all hospitalized (inpatient/emergency department) adult patients (older than 18 years of age) who underwent FGLPs from June 1, 2016, to March 31, 2022, were retrospectively reviewed.
The primary indication to perform FGLPs was to administer intrathecal chemotherapy or sample the CSF to detect malignancy, infection, CSF opening pressure, and other diseases. As per the standard guidelines in the radiology department, most patients had at least 1 failed attempt at bedside LP. Direct FGLP was available for patients requiring intrathecal chemotherapy, myelography, or cisternography and for patients with pre-existing conditions, such as morbid obesity, that could substantially reduce the chance of a successful non-image-guided LP. The decision to forgo a non-image-guided LP attempt was determined by the supervising neuroradiologist, similar to methods in other institutions.14
Data Collection
Data were collected retrospectively by 1 neuroradiology fellow through month-by-month review of FG spinal punctures performed in a 1 neurointerventional suite by reviewing our imaging database (Centricity; athenaIDX). All radiology reports of unsuccessful FGLPs from June 1, 2016, to March 31, 2022, were analyzed, and the clinical indication, demographic data, spinal levels at which the LP was attempted, training year of the operator, reason for failure, and whether the patient returned for another FGLP attempt (within 1 month) were documented from the radiology report.
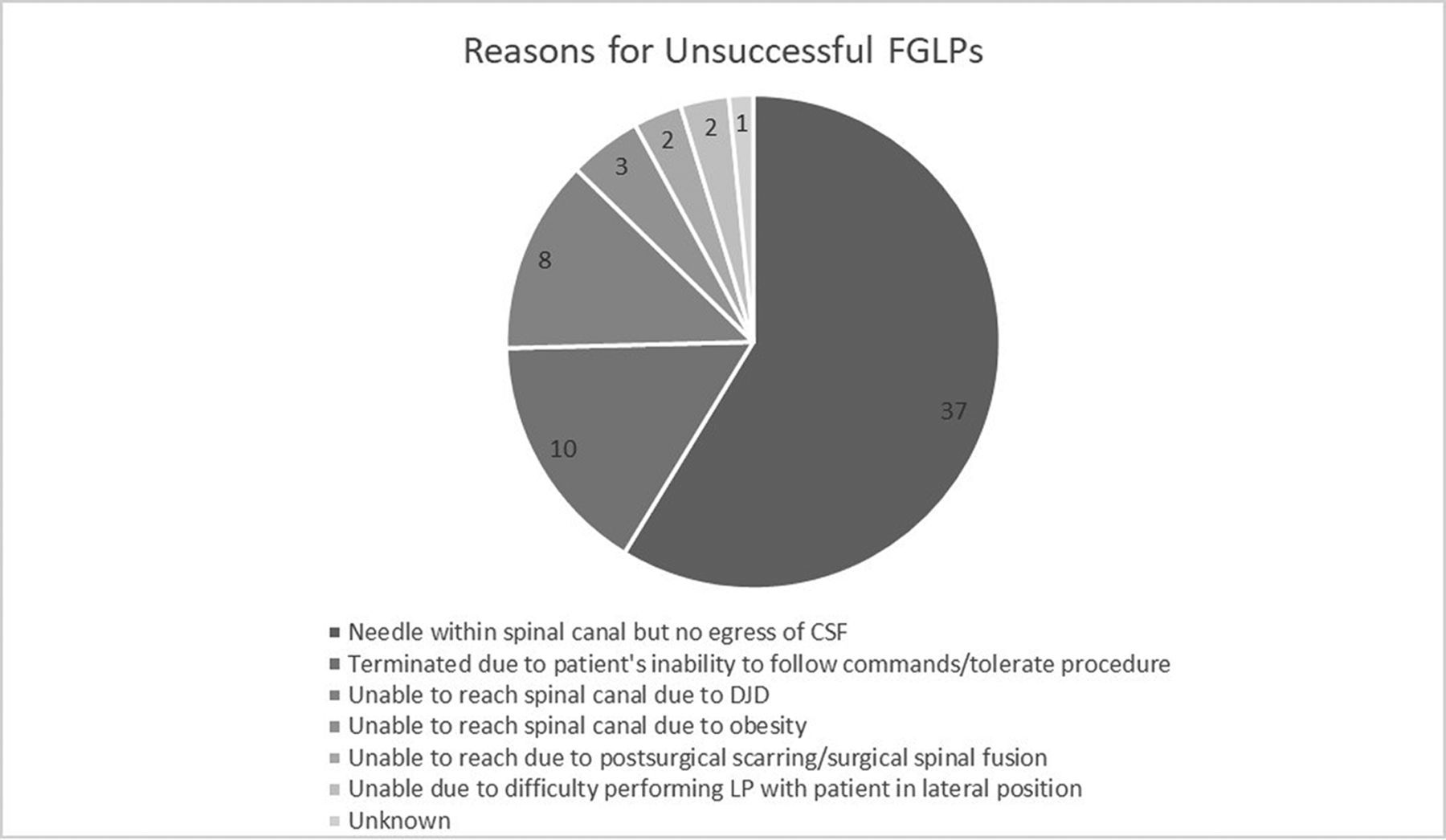
Unsuccessful FGLPs were cases with an inability to enter the spinal canal evidenced by lack of CSF egress and on fluoroscopy; an inability to collect CSF in tubes even though the needle was confirmed to be in the spinal canal on fluoroscopy; or for patient-related factors including the patient requesting termination of procedure due to pain, discomfort, or anxiety or the patient being confused and not able to follow directions or lie still. Figure 1 summarizes reasons for failure. We recorded the number of days between the initial and second FGLP attempts.

Breakdown of reasons for unsuccessful FGLPs. DJD indicates degenerative joint disease.
For patients with an initial failed FGLP due to a dry tap, we analyzed their clinical charts to determine whether they received IV fluids; specifically, we determined whether the clinician’s note mentioned starting or continuing IV fluids to assure success of a repeat FG spinal puncture, and/or we looked at the patient’s order set to ensure that patient received IV fluids. For patients with failures due to a high body mass index (BMI), we recorded their BMI obtained on the closest date to the first FGLP attempt. For patients who had initial failed FGLPs due to patient-related factors including discomfort, anxiety, and so forth, we determined whether the patient received antianxiety or pain medication or anesthesia before the repeat FG spinal puncture.
We reviewed pertinent clinical information for patients who did not return for a repeat FGLP to determine whether additional tests or procedures were performed as a substitution for an image-guided LP, such as infusion of chemotherapy through a shunt reservoir.
Data Analysis
The age and sex of study participants were described using descriptive statistics. To assess the relationship between the patient’s age, sex, lumbar levels attempted, resident’s training year, and clinical indication to undergo LP and the likelihood of patients returning for repeat spinal puncture compared with patients who did not return following a failed LP, we fit logistic regression models with 95% profile likelihood confidence intervals. P values < .05 were considered statistically significant.
RESULTS
From June 1, 2016, to March 31, 2022, 1389 FGLPs were performed on inpatients or patients in the emergency department. Sixty-three of 1389 (4.5%) patients (mean age = 59.8 [SD, 16.2] years; range = 18–93 years; median = 62 years; 55% women and 45% men) had failed initial attempts by 39 trainees at obtaining CSF. Sixty of 63 (95.2%) FGLPs were attempted under supervision of an attending, while the remaining 3 were performed by the resident during the weekend or weekday after hours. Of the 63 failed attempts, 21 failures were by R1s, 10 by R2s, 17 by R3s, 7 by R4s, 4 by neuroradiology fellows, and 4 failures were by 2 residents who were performing the FGLP together. The median failure rate was 1 per resident (range = 1–4 failures). Lumbar level-by-level failure rates on an initial attempt in the 63 patients were as follows: sole attempts at L2–3 = 3 (4.8%), L3–4 = 15 (23.8%), and L4–5 = 7 (11.1%); 2 levels attempted (L1–2 and L5–S1) = 23 (36.5%); and 3 levels attempted (L2–3 and L5/L6/S1) = 11 (17.5%). For 4 patients (6.3%), it was unclear which levels were attempted, but for 3, it was likely at 1 level. Patients’ clinical indications for the FGLPs were the following: concern for infectious process in the CSF = 25 (39.7%), concern for a neoplasm in the CSF = 15 (23.8%), testing for normal pressure hydrocephalus = 2 (3.2%), and all remaining categories including concern for MS, encephalitis, and so forth = 21 (33.3%).
Twenty-eight of 63 patients (61% women and 39% men, mean age = 58.6 [SD, 18.1] years, median = 64 years) returned to undergo a second FG spinal puncture (5 cervical and 23 lumbar approaches; mean = 4 [SD, 5.9] days after the first FGLP attempt, median = 2 days, range = 1–28 days). Twenty-seven of 28 (96.4%) had a successful repeat FG spinal puncture.
Failure Due to Lack of Egress of CSF through the LP Needle Confirmed in the Spinal Canal on Fluoroscopy
Thirty-seven of 63 (58.7%) failures were due to lack of egress of CSF through the LP needle, though the needle tip was within the spinal canal (46% women and 54% men, mean age = 59 [SD, 17.3] years, median age = 61 years, age range = 18–92 years). The mean lumbar spinal levels attempted on the initial failed FGLP were 1.9 (SD, 0.76) levels, median = 2 levels. A sole approach at levels L2–3 was 2 (5.4%); L3–4, 7 (18.9%); and L4–5, 4 (10.8%). Twenty-four patients (64.9%) had attempts at multiple levels. For 33 patients (89.2%), FGLP was attempted with the patient in the prone position and 1 patient was in the lateral position, and for 3 patients, positioning was unknown.
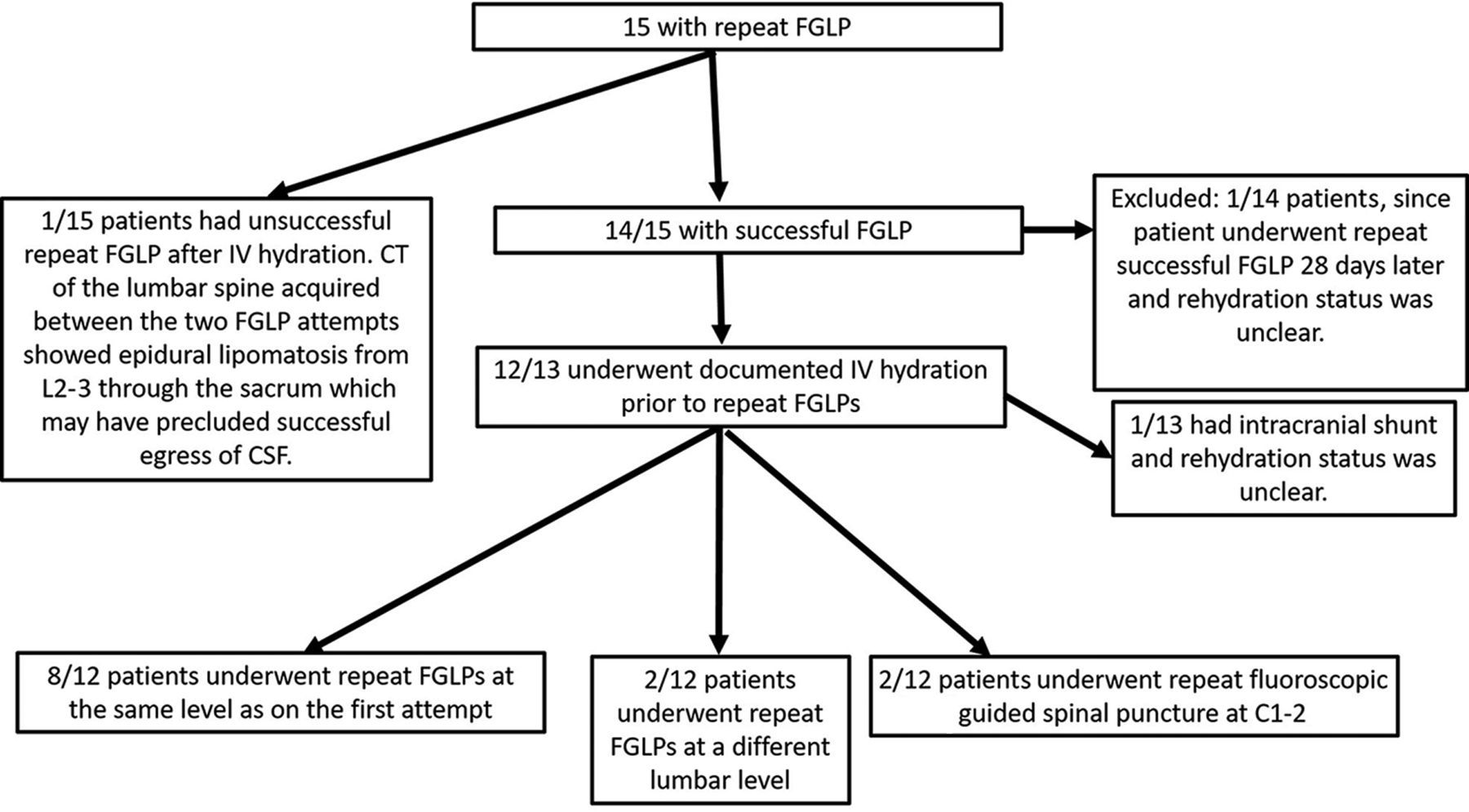
Fifteen of 37 patients (40.5%) (47% women and 53% men, mean age = 57.7 [SD, 18.6] years, median age = 64 years, age range = 18–82 years) returned to undergo FGLP at another date (mean = 4.7 [SD, 7.5] days, median = 2 days, range = 1–28 days) after the first attempt, of which 14/15 (93.3%) had a successful repeat FGLP. See Fig 2 for the breakdown.

Breakdown of patients with initial dry taps who returned for repeat FG spinal punctures.
Failure Due to Degenerative Changes
Eight of 63 (12.7%) failures were due to an inability to access the spinal canal due to degenerative changes as documented in the radiology report: 63% women and 37% men, mean age = 68.3 (SD, 9.8) years, median age = 65.5 years. The mean number of FGLP attempts at multiple lumbar levels after the initial failed FGLP was 2.4 (SD, 1.1), median = 2.
Two of 8 (25%) returned to undergo a repeat FGLP (range = 1–5 days after the first FGLP attempt). Both of these were successful and were performed at the C1–2 level.
Failure Due to Patients’ High BMI, Postsurgical Scarring, and Other Factors
High BMI.
Three patients had failed initial FGLPs due to an inability to adequately visualize the bony landmarks under fluoroscopy and an inability to reach to the spinal canal with the needle due to large body habitus (mean BMI = 48.3, range = 35.8–56.3). Two patients had initial FGLP attempts while in the lateral position either due to intubation or an inability to lie prone. One patient had a repeat successful non-image-guided LP on the inpatient floor, a second patient had a successful repeat FGLP with the use of a longer needle (14 days after the first failed FGLP), and the last patient did not have a repeat LP attempt and went for brain biopsy.
Postsurgical Scarring or Instrumentation.
One patient had a failed FGLP due to the inability of the LP needle to pierce through the postsurgical scarring in the lumbar spinal soft tissues. A repeat FGLP was not attempted because the patient’s symptoms resolved. One patient had a failed FGLP due to lumbar instrumentation. The patient underwent a successful cervical puncture the following day.
Other Factors.
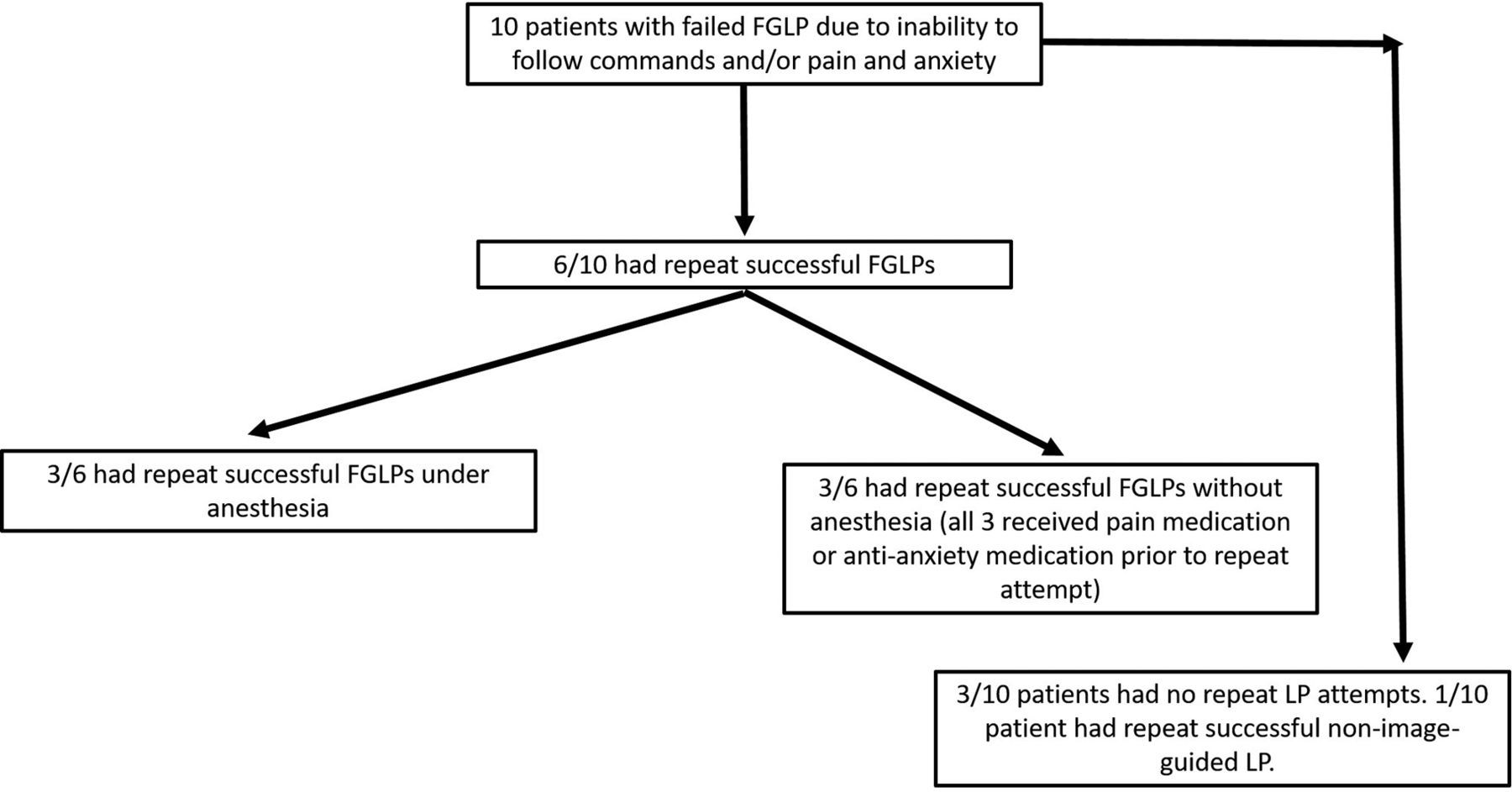
Ten patients had initial failed FGLPs due to an inability to follow commands and/or pain and anxiety. Six of 10 patients returned to undergo a repeat FGLP (mean = 2.2 [SD, 1.5] days, median = 2 days). See Fig 3 for outcomes.

Outcomes of patients with initial failed FGLPs due to an inability to follow commands and/or pain and anxiety.
Two patients had initial unsuccessful attempts while in the lateral decubitus position and 1 and 3 days later had successful FGLPs (1 under anesthesia). For 1 patient, the reason for the initial FGLP failure could not be determined, and the patient had a subsequent successful FGLP 2 days later. The Table 1 summarizes some of the data presented above.
Breakdown of data on failed and repeat spinal punctures
Factors Associated with Patients Returning for a Repeat FGLP Attempt
No clear relationship (P < .05) was seen regarding multiple factors and whether the patient returned for a repeat FGLP (Table 2).
Factors associated with whether the patient will return for a repeat FGLP and the reason for the failed LP
Patients Who Did Not Return for Repeat FGLP Attempts
Of the 35 patients who did not return for an FG spinal puncture, 5 had substitute procedures to determine the cause of their symptoms or to instill intrathecal agents, including placement of an Ommaya reservoir or other type of intracranial shunt or brain biopsy. One patient died from hypotension and hypoxia the day following the unsuccessful FGLP attempt, and the primary cause of death was ruled lymphoma. Two patients underwent successful LP attempts on the inpatient floor without image guidance.
The remaining 27/63 (43%) patients (52% men and 48% women, mean age = 59.2 [SD, 15] years, median = 62 years) did not undergo a further FGLP attempt because they improved clinically, other reasons for symptomatology were revealed, or the patient declined, among others. One hundred percent of the patients were successfully discharged to home or a care facility (median = 5 days, range = 0–16 days after admission).
DISCUSSION
Our findings, obtained from a large academic hospital, demonstrate a success rate of 95.5% FGLPs on the first FGLP attempt and 96.4% (27/28) after patients returned for a second fluoroscopically guided cervical or lumbar puncture. Success rates are higher compared with a non-image-guided approach, ∼72%,1 and a sonographically guided approach, 90%,16 primarily related to the ability to clearly visualize osseous structures and advancement of the LP needle in real time. Our success rate was slightly lower than the 99% success rate reported in another article with a smaller sample;2 the reasons could be multifactorial, including differences in the patient population and procedural expertise. Although in our study and the prior study, the miss rate was low, it is still important to analyze because FG spinal puncture is typically the last remaining option in many patients to obtain CSF, and if it is unsuccessful, it could directly impact their care. Furthermore, planning and performing FGLPs can be time-intensive6,10 and impact workflow as well as residency training in diagnostic neuroradiology;11 therefore, knowledge of potential reasons for failure is critical. Most important, our findings show that even if initially unsuccessful, repeat FG spinal punctures have a high success rate of 96% and can be reassuring for patients, ordering clinicians, and radiologists.
In our sample, most of the failed FGLPs were due to lack of egress of CSF through the LP needle, even though the needle tip was confirmed in the spinal canal and demonstrated no kinking, which could preclude outflow of CSF, ie, a dry tap. A prior article with a smaller sample size and conducted at another institution demonstrated that most of the FGLP misses, 44%, were due to dry taps,2 which is slightly lower than our findings (58.7%). Dry taps are believed to be due to low CSF volume and pressure, often due to dehydration.4 In our experience, ordering clinicians are aware that patients need to be hydrated before FGLPs, and we often specifically request that hospitalized patients are hydrated before the FGLP attempt. Even so, 37 patients in our sample still had initial dry FGLP taps. We followed the same maneuvers to acquire CSF as suggested by Hudgins et al;4 however, we do not use the “gentle suction” technique using a syringe, primarily due to procedural inexperience. Using this technique may provide some CSF flow but often remains slow.4 Many patients require ≥10 mL of CSF for proper analysis, and collecting adequate CSF, if egressing is slow, may be impractical because many relatively ill, elderly, and/or obese patients cannot remain in position for an extended time.
Of the 15 hospitalized patients who returned for a repeat FGLP while still hospitalized, 13 had documented IV hydration and 12 had successful FGLPs. Most had a repeat attempt at the same lumbar level as on the initial attempt. Imaging in the sole patient with the unsuccessful FGLP demonstrated epidural lipomatosis from L2–3 through the sacrum, which likely precluded successful egress of CSF because epidural lipomatosis a known factor for failed LPs.17 The patient was subsequently discharged because symptoms had resolved.
In 8 patients, the lumbar spinal canal could not be accessed due to degenerative changes. Most of these patients were older than 65 years of age, and advanced age is highly associated with degenerative disease of the lumbar spine.18 Only 2 patients returned for a repeat attempt and underwent successful cervical spinal punctures. Although not often performed, cervical spinal punctures remain a viable option to access the spinal canal for CSF sampling and/or myelography.19,20 If operators do not feel comfortable performing cervical punctures, accessing the spinal canal under CT guidance is an alternative option,4 though it results in an increase in the radiation dose. The percentage of unsuccessful FGLPs due to degenerative changes was overall low because fluoroscopy generally well-defines the spinal canal entry sites, typically the interlaminar or interspinous spaces.
A high BMI is a known factor for failed non-image-guided LPs.21 Even under fluoroscopy, due to increased soft tissue in the flank, ensuring a straight entry into the spinal canal can be difficult. Most interesting, only 3 patients had FGLP failures, primarily due to the patient’s high BMI. Our high success rate in patients with high BMIs is likely because we measure the skin-to-midspinal canal distance on CT or MR imaging before performing FGLPs to determine the correct needle length. If no prior imaging is available, we use the formula detailed by Nayate et al5 to determine the inches from the skin to the spinal canal.
FGLPs require patients to remain still for several minutes and can cause discomfort. Inpatients are often ill and cannot follow directions or remain still, are anxious, and cannot bear the discomfort. Clinicians strive to avoid unnecessarily sedating patients, and often the initial FGLP is attempted on patients and is subsequently terminated due to reasons stated above. In our sample, in only 10 patients did the initial FGLP attempts fail for reasons stated above. This low number is likely because we typically discuss the case with the ordering physician and ask if the patient can undergo the procedure without requiring sedation or anesthesia. Most of patients returned for a repeat FGLP (one-half with anesthesia and one-half without), and 100% had a repeat successful FGLP.
We hypothesized that most patients would return for a repeat FGLP. However, >40% of patients did not return for FGLPs because their symptoms resolved, patients declined further attempts, or they were planning to undergo FGLP as an outpatient. All of these patients were successfully discharged, typically a few days after the failed FGLP attempt. There was no difference between the likelihood of patients returning for a repeat FG spinal puncture or not based on the clinical indication. Of the approximately 44.4% of our sample that returned for a repeat FGLP, most returned within 2 days, which is expected because if there is concern for CSF pathologic processes, timely detection is needed for treatment planning and to reduce morbidity/mortality. Using this logic, we suspect that other radiology departments have similar referral timing for repeat FGLPs and therefore can adjust their FGLP schedule to allow return of these patients. An orderly functioning FGLP service is critical because FGLP referrals continue to increase3 and occupancy of a FGLP procedure room can be an hour or longer.6
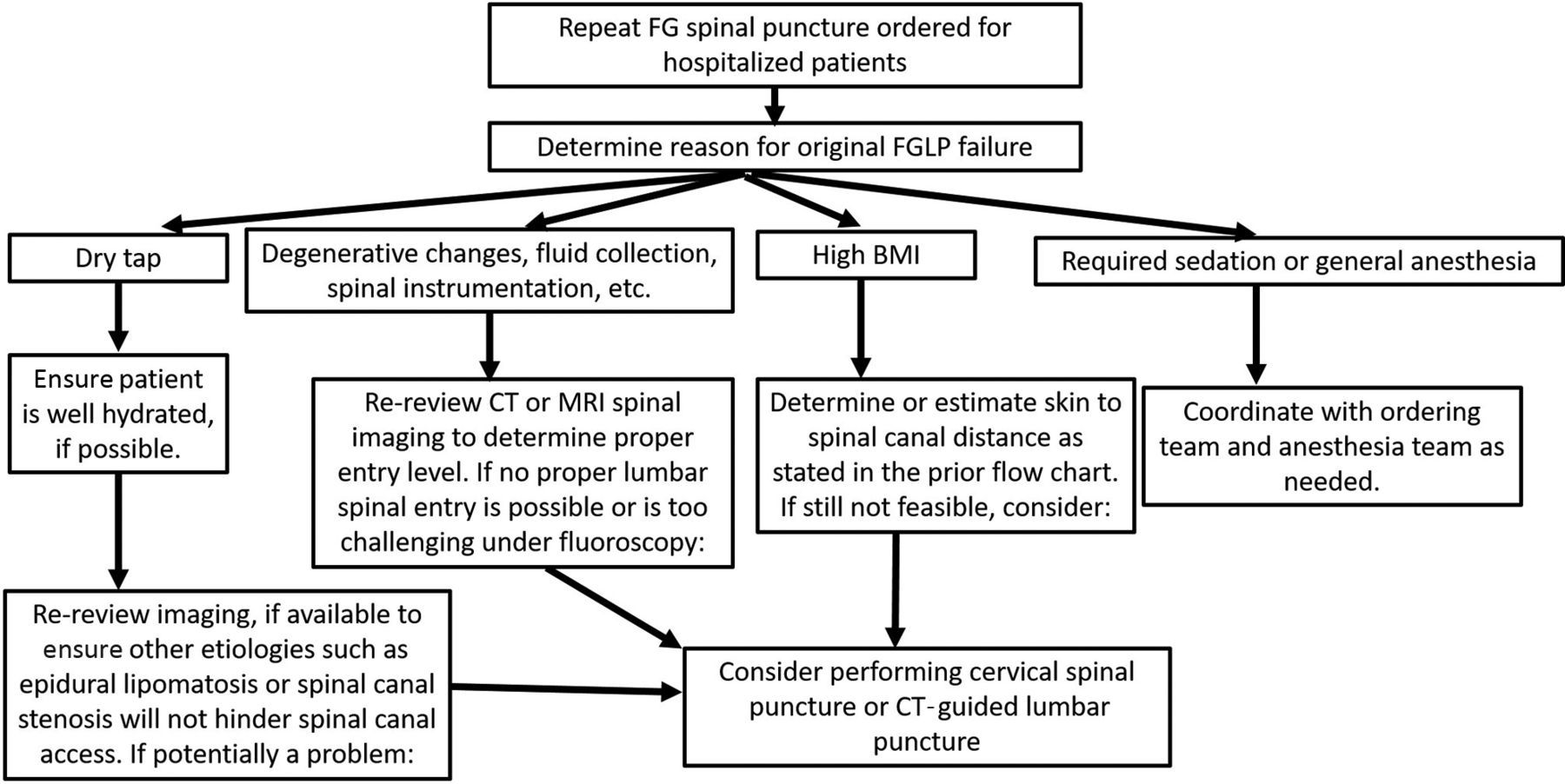
Well-organized scheduling, planning, and performing of FGLPs can sometimes be challenging; therefore, we have provided a flowchart (Figs 4 and 5) that can be followed to potentially ease the process.

Flowchart to determine how to prepare for and perform an FG spinal puncture. PO indicates by mouth.

Flowchart for patients who return for a repeat FG spinal puncture.
Our study has some limitations. First, our findings are based on the FGLPs performed at a single institution; although 39 trainees performed FGLPs under the supervision of 7–12 attendings, there was a broad range of operator skill. Our hospital is a tertiary academic center, and our radiology department performs FGLPs on patients with a large range of BMIs, medical conditions, degenerative changes, and other patient-related factors that are typically seen in hospital systems that service a substantial patient population. Second, we had a small sample size, but the high success rate of the repeat FGLPs supports our findings and assertions. Third, in some patients, multiple factors could have caused the failed FGLP attempt, but we focused on the primary cause as stated in the dictation and after review of the FGLP procedural images and patients’ charts. Fourth, we did not review CT or MR imaging of the lumbar spine in all patients to determine degree of degenerative changes because grading degenerative changes is often subjective and not standardized. Fifth, we did not objectively determine which patients with dry taps were initially dehydrated nor determine the amount of IV fluid they received because it is beyond the scope of this article but is the focus of our next research project.
CONCLUSIONS
We demonstrated a 95.5% success rate for FGLPs performed at our tertiary academic hospital and a near-equivalent success rate for patients who returned to undergo a second FG spinal puncture attempt after an initial failed FGLP attempt. Patients had a repeat FG spinal puncture within a median of 2 days after the initial failed attempt. A dry tap was the most common reason for a failed FGLP, and most patients had a successful FGLP after they were hydrated. More than 40% of patients did not require a repeat FGLP because their symptoms resolved, the patient declined further attempts, or other reasons for their symptoms were determined, which no longer required CSF sampling. There was no difference in the likelihood of patients returning for a repeat FG spinal puncture based on the clinical indication.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
ReferenceS
- Received November 21, 2022.
- Accepted after revision April 11, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.