
Abstract
BACKGROUND AND PURPOSE: Volumetric TSE (3D-TSE) techniques are increasingly replacing volumetric magnetization-prepared gradient recalled-echo (3D-GRE) sequences due to improved metastasis detection. In addition to providing a baseline for assessing postcontrast enhancement, precontrast T1WI also identifies intrinsic T1 hyperintensity, for example, reflecting melanin or blood products. The ability of precontrast 3D-TSE to demonstrate intrinsic T1 hyperintensity is not clear from the literature; thus, this study compares precontrast 3D-TSE and 3D-GRE sequences for identifying intrinsic T1 hyperintensity in patients with metastatic melanoma.
MATERIALS AND METHODS: Patients with metastatic melanoma and previously reported intrinsic T1 hyperintensity were identified. MRIs were performed at 3T including both 3D-GRE (MPRAGE) and 3D-TSE T1 sampling perfection with application-optimized contrasts by using different flip angle evolution (T1-SPACE) sequences precontrast. Axial 1-mm slices of both T1WI sequences were independently reviewed by 2 neuroradiologists, comparing the conspicuity of each lesion between the 2 sequences according to a 5-point scale and assessing whether the intrinsic T1 hyperintensity was attributable to melanin, blood products, or both.
RESULTS: Twenty examinations were performed, with a total of 214 lesions demonstrating intrinsic T1 hyperintensity. Both readers found that intrinsic T1 hyperintensity was less conspicuous with T1-SPACE compared with MPRAGE for most lesions assessed (81.8%, averaged across both readers), including for lesions with intrinsic T1 hyperintensity attributable to melanin and blood products. Intrinsic T1 hyperintensity was rarely more conspicuous on T1-SPACE (1.4%).
CONCLUSIONS: Precontrast intrinsic T1 hyperintensity is more conspicuous with MPRAGE than T1-SPACE. In patients with metastatic melanoma, 3D-GRE should be preferred as the precontrast T1WI sequence when both 3D-TSE and 3D-GRE are performed postcontrast and when not administering IV contrast.
ABBREVIATIONS:
- 3D-GRE
- volumetric magnetization-prepared gradient recalled-echo
- 3D-TSE
- volumetric TSE
- IMM
- intracranial melanoma metastases
- T1H
- intrinsic T1 hyperintensity
- T1-SPACE
- T1 sampling perfection with application-optimized contrasts by using different flip angle evolution
Volumetric TSE (3D-TSE) techniques are increasingly replacing volumetric magnetization-prepared gradient recalled-echo (3D-GRE) sequences such as MPRAGE for postcontrast T1WI, due to their improved ability to detect small intracranial metastases.1 For example, 1 important advantage of 3D-TSE over 3D-GRE is inherently greater suppression of normal vessels, which can otherwise obscure small metastases adjacent to vessels.2 Performing precontrast T1WI is important to confirm that hyperintensity demonstrated on postcontrast T1WI truly reflects enhancement rather than intrinsic T1 hyperintensity (T1H), and providing such a baseline is arguably the most important role of precontrast T1WI. The pre- and postcontrast sequences are typically performed with the same imaging parameters, to most accurately assess postcontrast enhancement.
The identification of T1H on precontrast T1WI is also important, given the limited number of possible causes, including melanin, blood products (methemoglobin), lipid, protein, and minerals (including calcification).3 Given its ability to identify melanin, precontrast T1WI plays a more important role in the assessment of metastatic melanoma as opposed to metastatic disease from other primaries. This role may be particularly relevant when using 3D-GRE because intracranial melanoma metastases (IMM) can occasionally be obscured by normal vessels on postcontrast imaging but be visible precontrast on the basis of T1H. T1H attributable to melanin occurs in approximately one-third of IMM,4,5 and the frequency of T1H attributable to melanin may be slightly higher in metastases with a BRAF mutation compared with BRAF wild-type disease.5 IMM also have a particular propensity to hemorrhage, which is more frequent than metastases from most other primaries.6 Both melanin and blood products may contribute to T1H within a given intracranial melanoma metastasis; thus, it is important to correlate precontrast T1WI with a susceptibility-sensitive sequence to aid in this distinction:5,7 Blood products will result in low signal on SWI,7 while melanin will produce either high signal due to the T1 shinethrough effect8 or intermediate signal.
With the transition from 3D-GRE to 3D-TSE for postcontrast T1WI, it follows that a similar transition will also occur for precontrast T1WI. However, the ability of precontrast 3D-TSE to detect T1H, in particular T1H attributable to melanin or hemorrhage, has not been assessed to our knowledge. If a single postcontrast T1WI sequence is performed, the precontrast T1WI sequence would generally be performed with the same parameters. There is, however, value in performing both 3D-TSE and 3D-GRE postcontrast, to optimize both the sensitivity and specificity for the detection of metastases.9 With such an imaging protocol, 1 precontrast T1WI sequence is adequate, but it is not clear from the literature whether 3D-TSE or 3D-GRE should be selected. In addition, gadolinium administration is contraindicated in some patients, and some patients may decline contrast administration, for example due to concerns regarding gadolinium accumulation. Therefore, the relative performance of the 2 T1WI sequences is an important consideration in clinical practice. The purpose of the study was to compare the identification of T1H in IMM on precontrast 3D-GRE and 3D-TSE.
MATERIALS AND METHODS
Patient Identification
Approval from the Peter MacCallum Cancer Centre ethics committee was obtained. Patients were identified prospectively on the basis of an upcoming MR imaging booking and a history of metastatic melanoma. All were adult patients. The preceding MR imaging report for each patient was reviewed by the lead study neuroradiologist (with 10 years of subspecialty expertise in neuro-oncology), and patients in whom T1H was reported were identified. Verbal consent for the additional sequence was obtained from each patient following an institutional ethics committee–approved procedure. A total of 20 examinations were planned.
Image Acquisition
All MR imaging examinations were performed on 3T MR imaging (Magnetom Skyra; Siemens) using a standardized protocol, including pre- and postcontrast 3D-GRE (MPRAGE), precontrast 3D-TSE (T1 sampling perfection with application-optimized contrasts by using different flip angle evolution [SPACE sequence; Siemens]), axial T2WI, axial FLAIR, DWI, and SWI. T2WI was performed between contrast administration and postcontrast MPRAGE. MPRAGE was performed in the axial plane. The parameters for MPRAGE were the following: TR = 1900 ms; TE = 2.44 ms; TI = 944 ms; flip angle = 8°; frequency = 6; phase = 256; number of excitations = 1; FOV = 256 mm; section thickness = 1 mm; fat suppression = water excitation; parallel imaging acceleration factor = 2; bandwidth = 250 Hz/px. Initially, T1-SPACE was also performed in the axial plane (for the first 7 examinations), but wrap-around artifacts occurred in the superior aspect of the FOV in some patients. As a result, the acquisition plane was changed to sagittal (for the remaining 13 examinations), though images were primarily assessed in the axial plane with 1.0-mm section thickness, to be equivalent to MPRAGE. The parameters for T1-SPACE were the following: TR = 700 ms; TE = 11 ms; frequency = 256; phase = 256; number of excitations = 1.4; FOV = 256 mm; section thickness = 1 mm; fat suppression = fat saturation strong; blood suppression = free; parallel imaging acceleration factor = 2; bandwidth = 630 Hz/px. Both sequences were similar in duration: 3 minutes and 44 seconds for MPRAGE and 4 minutes and 4 seconds for T1-SPACE. Examinations were performed between February and October 2020.
Imaging Review
All MR imaging examinations were first assessed by the lead study neuroradiologist, either at the time of the initial report (n = 5) or later, but blinded to the report (by nonstudy radiologists; n = 15). Axial 1-mm slices of both T1WI sequences were reviewed, comparing the conspicuity of each lesion between the 2 sequences according to a 5-point scale: similar to that used previously by Goncalves Filho et al10 for the detection of gadolinium-enhancing lesions with different T1-SPACE sequences: only visualized on T1-SPACE; visible on MPRAGE but better visualized on T1-SPACE; similar conspicuity on both sequences; visible on T1-SPACE but better visualized on MPRAGE; or only visible on MPRAGE. SWI was also assessed to determine whether the T1H could potentially be solely attributed to blood products, solely attributed to melanin, or mixed (with both magnetic susceptibility and at least a portion demonstrating T1H without associated magnetic susceptibility). Examples are shown in Fig 1. Lesion locations (anatomic locations and image numbers) were noted, and the MRIs were subsequently reviewed by a second neuroradiologist (with >20 years of experience) in the same way, blinded to the first reader's assessment and the clinical report. Assessment was performed using the standard clinical PACS in a typical reading room environment. The window and level were determined by each reader on a case-by-case basis.

SWI (left column), precontrast T1-SPACE (middle column), and precontrast MPRAGE (right column) images demonstrating the determination of the cause of T1H. In the first patient (A–C), there is a small intracranial melanoma metastasis (arrowheads) at the medial margin of the right paracentral lobule demonstrating T1H (B and C), but no magnetic susceptibility (A), thus consistent with melanin. A cerebellar vermian lesion (dotted circles) with central T1H in the second patient (D–F) demonstrates magnetic susceptibility throughout the lesion (D), thus the T1H is potentially entirely attributable to blood products. In the third patient (G–I), there is a small area of magnetic susceptibility at the anteromedial aspect of the lesion (G, arrow), but the remainder of the T1H (H and I, arrows) does not have associated magnetic susceptibility, consistent with a combination of melanin and blood products. In all 3 examples, the T1H is similarly conspicuous on T1-SPACE as MPRAGE.
Statistical Analysis
The Fleiss κ was computed to assess the agreement between the 2 MR imaging readers for determining the nature of T1H and the relative conspicuity between the 2 sequences, according to categoric scales (nominal and ordinal, respectively). When determining the nature of T1H, lesions that could not be confidently characterized due to artifacts were excluded. T1-SPACE and MPRAGE were compared using the exact binomial test, considering together lesions better seen on 1 particular sequence and only seen on that sequence. All statistical analyses were performed in R statistical and computing software (Version 4.0.3; http://www.r-project.org/) using standard and validated statistical procedures.
RESULTS
Twenty MRIs including precontrast 3D-TSE were performed, in a total of 18 patients (2 patients had 3D-TSE on 2 separate occasions within the study period). There were a total of 214 lesions demonstrating T1H, with a median of 2 per examination (range, 1–141 lesions). The median age of the 18 patients (obtained at the time of the first examination for the 2 patients with 2 study examinations) was 58 years (range, 27–87 years), with an equal number of men and women. Five patients had presented with metastatic disease of unknown primary; 4 had lower limb primaries; 2 each had primaries on their neck, back, and chest wall; and the remaining 3 patients had primaries in other locations (shoulder, ear, and conjunctiva). These background data are summarized in Table 1.
Background data
Both readers determined that T1H was attributable solely to melanin for most lesions (179 and 170 lesions, respectively, for the 2 readers). Both melanin and blood products were demonstrated in 4.7% of lesions (taking the average of the 2 readers' results), while T1H could be entirely attributed to blood products in an average of 11.2% of the lesions. Only in a minority of lesions was SWI unable to adequately characterize the T1H due to artifacts, generally due to a peripheral location. Further detail is provided in Table 2. There was good interobserver agreement for assessing the cause of T1H (Fleiss κ = 0.71, P < .001).
MR imaging assessment results for both readers
Both readers determined that more than half of the lesions were better visualized on MPRAGE but were visible on T1-SPACE (57.2% of the lesions averaged across the 2 readers), with a further 24.5% seen only on MPRAGE. Overall, 81.8% of lesions were better visualized on MPRAGE than on T1-SPACE (P < .0001), while conspicuity was similar on both sequences for 16.8% of lesions. It was rare for lesions to be better seen on T1-SPACE: According to reader 1, one lesion was more conspicuous on T1-SPACE and another was seen only on T1-SPACE; and for reader 2, four lesions were more conspicuous on T1-SPACE and none were seen only on T1-SPACE. These results are also summarized in Table 2. Some examples of the differences in conspicuity are shown in Fig 2. Interobserver agreement was moderate (Fleiss κ =0.59, P < .001) for comparing the conspicuity of T1H on T1-SPACE and MPRAGE. The discrepancies were largely one reader assessing the lesion as being better seen with MPRAGE and the other reader assessing the lesion as seen only on MPRAGE, or one reader assessing the lesion as being better seen with MPRAGE and the other reader reporting similar conspicuity. Table 3 has additional data on the interobserver agreement for comparing T1-SPACE and MPRAGE.

Precontrast T1-SPACE (left column) and precontrast MPRAGE (right column) images demonstrating differing conspicuity of IMM. In the first patient (A and B), 2 IMM (arrows) are less conspicuous on T1-SPACE (A) compared with MPRAGE (B). In another patient (C and D), a right frontal cortical intracranial melanoma metastasis (arrowhead) is more conspicuous on T1-SPACE (C) than on MPRAGE (D), albeit subtle on both sequences.
Interobserver agreement for comparing the conspicuity of T1H between T1-SPACE and MPRAGE
Lesions were also divided into those with evidence of only melanin or only blood products (excluding lesions with evidence of both or indeterminate due to artifacts). For lesions with T1H attributable to melanin, reader 1 assessed 88.8% of lesions as being more conspicuous with MPRAGE (including those only seen on MPRAGE), with 81.8% for reader 2. For lesions with T1H attributable to blood products, reader 1 reported that MPRAGE better visualized the lesion in 73.1%, and reader 2, in 69.6%. These results are also included in Table 2. In all 12 examinations demonstrating >1 lesion with T1H, the conspicuity of individual lesions varied to some extent, as assessed by both readers.
DISCUSSION
Both readers independently determined that MPRAGE is overall better than T1-SPACE for identifying T1H. Not infrequently, the difference between the 2 sequences was quite marked (Fig 2), supporting the well-accepted recommendation of using the same T1WI sequence both before and after contrast administration. Nevertheless, some centers may perform more limited T1WI precontrast (eg, single-plane axial or sagittal acquisition), and it is important to be aware of potential differences in signal due to technical factors. The lower conspicuity with T1-SPACE was particularly pronounced for lesions containing melanin but was also evident in most lesions with T1H due to blood products. The latter may be an advantage in some settings: The presence of T1H often makes it more difficult to appreciate postcontrast enhancement. This feature suggests that 3D-TSE may facilitate assessment of enhancement in hemorrhagic lesions, though we have not specifically investigated this possibility. Ultimately, our results provide valuable insights into the differences between the 2 sequences, in turn allowing the optimal sequence to be selected for the given scenario.
Despite the greater conspicuity on MPRAGE, the choice of the T1WI sequence is, in large part, dependent on the postcontrast T1WI sequence being used, and 3D-TSE has other important advantages over 3D-GRE as outlined above. However, if IV gadolinium is contraindicated or declined, our results indicate that unenhanced 3D-GRE is better than unenhanced 3D-TSE for detecting IMM. In addition to 3D-TSE producing generally lower conspicuity of T1H, its key advantages of over 3D-GRE for the assessment of metastatic disease, namely vascular suppression and more pronounced enhancement,2 are negated in the absence of IV contrast. Also, while more pronounced T1H from blood products that occurs with 3D-GRE may be a disadvantage when trying to assess postcontrast enhancement, it may be beneficial when IV contrast is not administered, especially if a susceptibility-sensitive sequence is not used.
Our findings are also relevant when contrast is administered. While a single postcontrast T1WI sequence is performed in many centers, there are benefits in performing both 3D-TSE and 3D-GRE postcontrast. 3D-TSE improves detection of intracranial metastases, especially small metastases,1,11 but has a higher false-positive rate due to incompletely suppressed vessels mimicking metastases,12 which is particularly relevant in patients without known intracranial metastatic disease.9 In contrast, the more pronounced vascular enhancement with 3D-GRE can obscure small metastases, but it allows the equivocal findings on 3D-TSE to be resolved, being able to distinguish between metastases and normal vessels.9,12 In our routine practice, we currently perform both 3D-TSE and 3D-GRE postcontrast, for the reasons outlined above, and consider performing a single precontrast T1WI sequence to assess enhancement adequately. For small IMM demonstrating T1H, it is not uncommon for these to be best identified on precontrast 3D-GRE due to relative obscuration by enhancing vessels on postcontrast 3D-GRE and the presence of less marked hyperintensity on postcontrast 3D-TSE (Fig 3). Therefore, when performing both 3D-GRE and 3D-GRE postcontrast in patients with metastatic melanoma, we recommend 3D-GRE precontrast rather than 3D-TSE. We also suggest value in performing 3D-GRE rather than 3D-TSE precontrast in patients with metastatic disease from an unknown primary because the greater conspicuity of T1H when using MPRAGE may allow melanoma to be suggested as the likely primary with greater confidence.

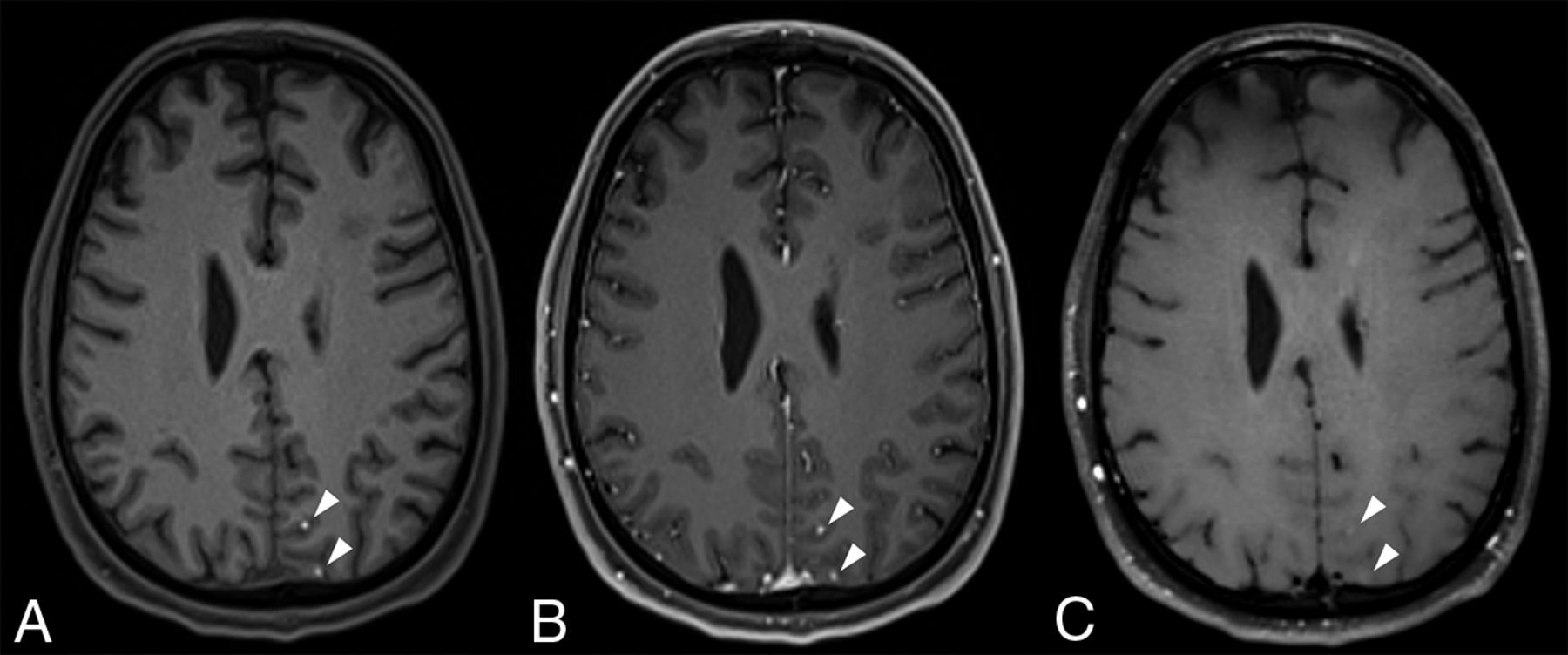
Precontrast MPRAGE (A), postcontrast MPRAGE (B), and postcontrast T1-SPACE (C) images showing 2 left parietal IMM demonstrating T1H (arrowheads), which are most conspicuous on the precontrast MPRAGE images (A). They are relatively less obvious on the postcontrast MPRAGE image (B) due to the enhancement of normal vessels and are barely visible on postcontrast T1-SPACE (C).
The reasons for the differences in the conspicuity of some lesions between the 2 sequences are not clear. They may not be entirely related to a visible difference in the T1 signal of the lesions, but, in part, to differences in the signal of the background brain parenchyma. Specifically, most small IMM are located at the interface between the cortex and the leptomeninges,13 in contrast to the gray-white matter junction location more typical of metastases from other primaries;14 and 3D-GRE inherently produces better gray-white matter differentiation than 3D-TSE.2 Thus, the relatively lower signal of the cortex with 3D-GRE facilitates the identification of T1H located within it, which may account for some of the differences in conspicuity, especially when lesions exhibit more subtle T1H. In some lesions, the coexistence of melanin and blood products may have also been a factor, given that a GRE technique is inherently more sensitive to blood products. We note that 3D-TSE was performed with fat saturation, as recommended in the aforementioned consensus guidelines.2 While it is not feasible to perform fat saturation with 3D-GRE sequences,2 a similar effect was achieved by performing MPRAGE with a water excitation technique.15 We consider it unlikely that the differences in fat-suppression techniques would affect the conspicuity of T1H, though we cannot be certain. Despite these additional considerations, our impression is that a component of the difference does indeed reflect greater sensitivity to melanin using a 3D-GRE technique.
There is the potential for selection bias in our study because patients were identified on the basis of T1H having been identified on previous 3D-GRE imaging, though we think that this feature would have had little effect, if at all. This was necessary logistically, given that only a minority of MR imaging examinations had evidence of T1H. Nevertheless, we think that identifying patients prospectively, before the study examination had been performed, would have been less prone to bias than a purely retrospective analysis.
CONCLUSIONS
T1H is overall more conspicuous with MPRAGE than T1-SPACE, both for melanin and blood products. Therefore, precontrast 3D-GRE should be preferred over 3D-TSE in patients with metastatic melanoma in whom both 3D-GRE and 3D-TSE are performed postcontrast or when not administering IV contrast, and it may aid in the diagnosis in patients with metastatic disease from an unknown primary. It is also important to be aware of potential differences in the appearances if using different T1WI sequences pre- and postcontrast.
Footnotes
Arian Lasocki was supported by a Peter MacCallum Cancer Foundation Discovery Partner Fellowship.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 2, 2022.
- Accepted after revision July 17, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.