
Abstract
BACKGROUND AND PURPOSE: Whether thrombus burden in acute ischemic stroke modify the effect of intravenous thrombolysis (IVT) before mechanical thrombectomy (MT) remains uncertain. We aim to investigate the treatment effect of stratified clot burden score (CBS) on the efficacy and safety of direct versus bridging MT.
MATERIALS AND METHODS: This is an exploratory subgroup analysis of a randomized trial evaluating the effect of CBS on clinical outcome in the DIRECT-MT trial. CBS was divided into 3 groups (0–3, 4–6, and 7–10) based on preoperative CTA, where higher scores indicated a lower clot burden. We report the adjusted common odds ratio for a shift toward better outcomes on the mRS after thrombectomy alone compared with combination treatment by stratified CBS groups.
RESULTS: No modification effect of mRS distribution was observed by CBS subgroups (CBS 0–3: adjusted common ratio odds 1.519 [95% CI, 0.928–2.486]; 4–6: 0.924 [0.635–1.345]; 7–10: 1.040 [0.481–2.247]). Patients with CBS 4–6 had a higher rate of early reperfusion (adjusted OR (aOR), 0.3 [95% CI, 0.1–0.9]), final reperfusion (aOR 0.5 [95% CI, 0.3–0.9]), and fewer thrombectomy attempts (aOR 0.4 [95% CI, 0.1–0.7]). Patients with CBS 7–10 had a higher rate of asymptomatic intracranial hemorrhage (14.9% versus 36.8%, P = .0197) for bridging MT. No significant difference was observed in other safety outcomes by trichotomized CBS.
CONCLUSIONS: The subgroup analysis of DIRECT-MT suggested that thrombus burden did not alter the treatment effect of IVT before MT on functional outcomes in CBS subgroups.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- aOR
- adjusted OR
- acOR
- adjusted common odds ratio
- CBS
- clot burden score
- eTICI
- expanded TICI
- ICH
- intracerebral hemorrhage
- IVT
- intravenous thrombolysis
- MT
- mechanical thrombectomy
Mechanical thrombectomy (MT) plus intravenous thrombolysis (IVT) has been the standard care for patients who have had acute ischemic stroke (AIS).1 IVT enhances the probability of early recanalization while carrying the risk of intracerebral hemorrhage. For large thrombus burden, IVT is believed to be less efficient because the rate of recanalization is low for occlusion of proximal large arteries.2⇓⇓⇓-6 In the meantime, a larger thrombus burden can lead to lower recanalization rates, worse clinical outcomes, and a higher risk of hemorrhagic complications.4,6,7 Therefore, IVT may exert a different treatment response to varying thrombus burden.
DIRECT-MT (Direct Intra-arterial Thrombectomy in Order to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals Multicenter Randomized Clinical Trial) is a multicenter randomized clinical trial to compare the efficacy of direct MT and bridging MT (MT plus IVT) in eligible patients with acute ischemic stroke, aiming to see whether IVT can be skipped before MT.8 We hypothesized that thrombus burden may impose a treatment effect on the functional and safety outcomes when applying bridging or direct MT for stratified thrombus burden. Hereby, we sought to examine the effect of stratified clot burden score (CBS 0–3 versus 4–6 versus 7–10) on the clinical outcomes in the subgroup analysis of DIRECT-MT.
MATERIALS AND METHODS
This is an exploratory analysis of the DIRECT-MT trial, a multicenter randomized clinical trial to determine whether direct MT was noninferior to bridging MT in patients with AIS due to anterior circulation large-vessel occlusion within 4.5 hours after stroke onset. The trial protocol and patient eligibility criteria have been previously published.8,9 In this secondary analysis, we divided CBS into 3 groups to investigate the treatment effect of CBS on the efficacy and safety of direct MT versus combined thrombolysis with MT.
Patients
The subgroup analysis was conducted within the intention-to-treat population. Patients who received randomization were enrolled in the subgroup analysis. The inclusion criteria for the DIRECT-MT trial included age ≥18 years, the occlusion of ICA together with the first or proximal segment of the middle cerebral artery on CTA, NIHSS ≥2, time window of 4.5 hours applicable to IVT. The exclusion criteria included mRS >2 or any contraindication to IV alteplase. Patients with missing data of CTA and graded CBS were excluded from the subgroup analysis. The functional outcomes were evaluated by an independent outcome assessment committee. The adverse event was judged by the adverse event committee. Written informed consent was obtained from each patient before randomization. The study protocol was approved by the hospital ethics committee and the research board of participating centers.
Stratification of CBS
CBS is a grading system of reflecting the extent and location of thrombus formation for semiquantitative analysis of thrombus burden for large-vessel occlusion in anterior circulation estimated on CTA.10 The value of CBS was graded by using the previously described algorithm.10 The purpose of CBS grading was to qualify the extent of intracranial thrombus, allotting 10 points for the presence of large arteries on CTA. For occlusion of each involved artery, corresponding points were subtracted from the total 10 points. The lower CBS signified a larger thrombus burden. To stratify the CBS rationally, the curve filling on the relationship of a favorable outcome, mortality, and CBS was validated. After binary logistic regression, we stratified the CBS into 3 subgroups: 0–3, 4–6, and 7–10 (Online Supplemental Data).
Outcome Measures
The radiologic outcomes were evaluated by the DIRECT-MT imaging core lab. All the imaging data were read by 2 independent readers from the core lab who were blinded to treatment allocation and final outcomes. A third reader provided a final adjudication in cases of discrepancies between the 2 readers. The required data regarding the baseline demographics, imaging results, time intervals, and functional and safety outcomes were retrieved from the locked database, and transferred to an independent statistician (X.Y.). The NIHSS was assessed at baseline, thrombectomy after 24 hours, and at 5–7 days or discharge. Early reperfusion before thrombectomy was defined as expanded TICI (eTICI) ≥2a on angiogram and successful reperfusion was defined as eTICI ≥2b. The clinical outcome was evaluated by means of mRS at 90 days, which was further classified as an excellent functional outcome of mRS 0–1, a favorable outcome of mRS 0–2, and a moderate outcome of mRS 0–3. Follow-up CT and CTA scanning were performed within 24–72 hours after endovascular treatment. Asymptomatic and symptomatic intracerebral hemorrhages (ICHs) were classified according according to the Heidelberg criteria.11 Procedural complications included any procedural complications, vessel dissection, contrast extravasation, and embolization in a new cerebrovascular territory. Contrast extravasation was defined as contrast leakage on intraprocedural dynamic angiograms.
The primary outcome was to estimate the treatment effect on the functional outcome in patients with stratified CBS by using multivariable ordinal regression to observe the adjusted common ratio odds (acOR) for the shift toward a better functional outcome of the mRS at 90 days for direct MT versus bridging MT. The secondary outcomes included functional and radiologic outcomes. The functional outcomes included the dichotomized mRS at 90 days, Barthel Index 95 or 100 at 90 days, NIHSS after 24 hours, and at 5–7 days or discharge. The radiologic outcomes included early reperfusion before thrombectomy (≥2a), final reperfusion of eTICI score ≥2b, the recanalization rate at 24–72 hours, midline shift, thrombectomy attempts, and the outcome lesion volume on postprocedural CT.
Safety outcomes were death, and asymptomatic and symptomatic ICH, which were classified according to the Heidelberg criteria.11 Procedural complications included any procedural complications, vessel dissection, contrast extravasation, and embolization in a new cerebrovascular territory. Contrast extravasation was defined as contrast leakage on intraprocedural dynamic angiograms.
Statistical Analysis
Normality of distributions was examined by using histograms and Shapiro–Wilk test. Data are presented as median (interquartile range) or as percentage. The baseline characteristics, functional and safety outcomes were compared by using the adjusted common odds ratio or χ2 test for categorical variables, Cochran-Mantel-Haenszel test for stratified categorical data, and Wilcoxon rank-sum test for non-Gaussian distributions by CBS subgroups. Univariate and multivariate regression analyses were performed to observe whether CBS was included as one of the independent prognostic factors that influenced the favorable outcome. The adjusted factors included age, ASPECTS, baseline NIHSS, baseline mRS, time from onset to randomization, collateral score, medical history, CBS, and treatment allocation.
To observe the treatment effect of IVT before MT on the functional outcome by CBS subgroups, multivariable ordinal regression analysis was performed to calculate the acOR for a shift in a direction toward a better functional outcome on the mRS at 90 days. Binary logistic regression was used to calculate the adjusted and unadjusted OR and 95% CIs for secondary outcomes to observe the modification or confounders effect based on CBS stratification, and adjusted and unadjusted relative risk and 95% CI for safety and serious adverse events outcomes. Linear regression was used to calculate adjusted and unadjusted β with 95% CIs for continuous outcomes. Interobserver agreement for trichotomized CBS was measured by using the weighted κ statistic with quadratic weighting.
The subgroup analysis was performed by using the SAS version 9.4 (SAS Institute) and R version 4.1.3 software package. A level of P < .05 was accepted as statistically significant.
RESULTS
The trial profile is shown in the Online Supplemental Data. In the DIRECT-MT trial, 656 patients under randomization, 641 patients were included for subgroup analysis, of whom 315 patients were allocated in direct MT group and 326 patients in bridging MT group. Among the 641 patients, 209 patients had CBS 0–3 (108 [51.7%] in direct MT group versus 101 [48.3%] in bridging MT group, and 347 had CBS 4–6 (direct MT: bridging MT; 160 [46.1%] versus 187 [53.9%]) and 85 had CBS 7–10 (direct MT: bridging MT; 47 [55.3%] versus 38 [44.7%]).
The baseline characteristics of the patients are summarized by CBS subgroups in the Online Supplemental Data. The median time from intravenous alteplase to groin puncture is 27 (interquartile range, 15–39) minutes. No significant difference was observed in the proportion of patients treated with direct or bridging MT between groups. We noticed a longer median time from groin puncture to reperfusion, from randomization to reperfusion, and from stroke onset to reperfusion in patients with lower CBS. However, no significant differences in the median time from stroke onset to IV alteplase, from stroke onset to reperfusion, or from intravenous alteplase to groin puncture were observed.
Patients with lower CBS had higher NIHSS scores, lower ASPECTS, worse collateral scores (combined grade 0–1, 87.9% of 206 patients with CBS 0–3; 75.3% of 340 patients with CBS 4–6; 61.4% of 83 patients with CBS 7–10), a higher incidence of cardioembolic sources on stroke etiology, a higher proportion of ICA occlusion, and longer time interval from admission to reperfusion, from groin puncture to reperfusion and from randomization to reperfusion (Online Supplemental Data). The time from stroke onset to groin puncture is slightly longer in patients with CBS 4–6. Univariate and multivariate logistic regression analyses showed that CBS was an independent prognostic factor for favorable outcomes (OR, 1.181 [95% CI, 1.064–1.312, P = .002]) (Online Supplemental Data).
The outcome of patients was summarized by CBS stratification between 2 groups in the Online Supplemental Data. We noted that patients with lower CBS had a worse degree of overall disability, a lower incidence of excellent, favorable, and moderate functional outcome, Barthel Index 95 or 100 at 90 days, and a higher median NIHSS after 24 hours and at 5–7 days or discharge. In the meantime, no difference in the rate of early reperfusion before MT and the recanalization rate at 24–72 hours was observed. Patients with lower CBS had a higher successful reperfusion rate (Online Supplemental Data).
The acOR for a better 90-day mRS was 1.5 (95% CI 0.9–2.5) for CBS 0–3, 0.9 (0.6–1.3) for CBS 4–6, and 1.04 (0.5–2.2) for CBS 7–10 in the direct MT group compared with the bridging MT group (Fig 1). There was no significant treatment-by-trichotomized CBS interaction for the ordinal mRS distribution (acOR interaction term relative to CBS 7–10: CBS 0–3, 0.73 [95% CI 0.30–1.81], P = .503; CBS 4–6, 1.06 [95% CI 0.45–2.48], P = .894) (Fig 2; Online Supplemental Data). No significant difference in the bridging effect was observed for dichotomized mRS, Barthel Index 95 or 100 at 90 days, NIHSS after 24 hours and 5–7 days, or discharge by CBS subgroups.

Treatment effect for mRS distribution shift on 90 days in trichotomized subgroups.

Treatment effect for mRS distribution shift on 90 days by treatment group in trichotomized subgroups.
In the adjusted analysis, patients with CBS 4–6 had a higher rate of early reperfusion (absolute difference 5.76%, adjusted OR (aOR) 0.3 [95% CI, 0.1-0.9]), final reperfusion (absolute difference 8.17%, aOR 0.5 [95% CI, 0.3-0.9]), and less thrombectomy attempts (aOR 0.4 [95% CI, 0.1-0.7]) in bridging MT group than direct MT group for patients with CBS 4–6. With respect to other secondary radiologic outcomes, we noted no significant treatment-by-trichotomized CBS interaction for the recanalization rate at 24–72 h on CTA, midline shift, and outcome lesion volume on CT (Online Supplemental Data).
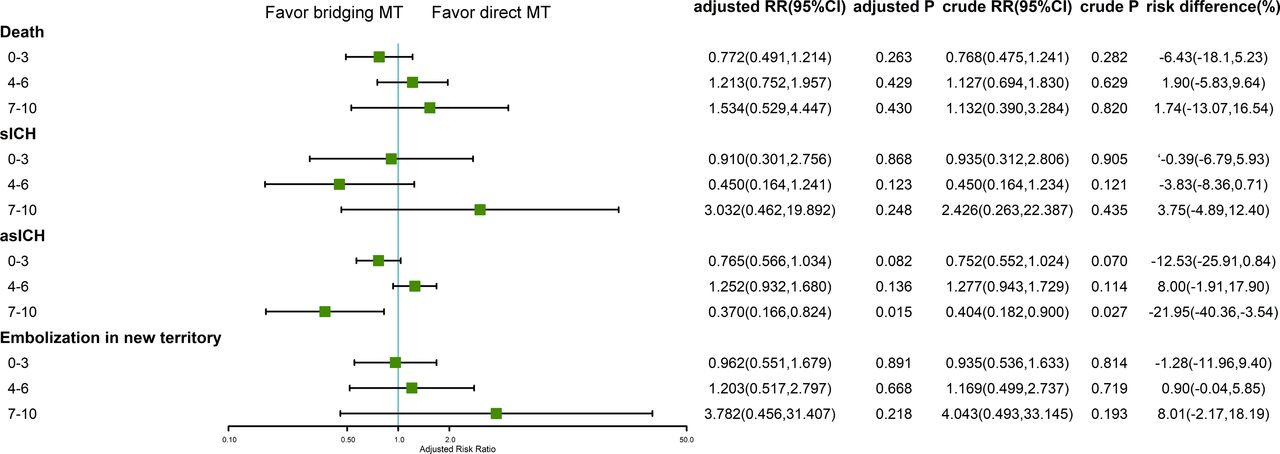
Patients with lower CBS had higher rates of mortality, asymptomatic ICH, midline shift, any procedural complication, and embolization into a new territory (Online Supplemental Data). We noted no significant difference in symptomatic ICH, vessel dissection, and contrast extravasation between CBS subgroups. With the exception of asymptomatic ICH, we noted no significant treatment-by-trichotomized CBS interaction for any of the other safety outcomes. The asymptomatic rate in the bridging MT group was higher than that in the direct MT group in patients with CBS 7–10 (OR, 0.279 [95% CI, 0.094–0.825], P = .0197) (Fig 3; Online Supplemental Data).

Safety outcomes by treatment group in trichotomized subgroups.
The observed agreement for trichotomized CBS was 588 (92%) of 636, yielding a weighted κ of 0.936 (SE 0.012). The concordance correlation coefficient for numeric CBS was 0.941 (95% CI 0.933–0.948).
DISCUSSION
The subgroup analysis of DIRECT-MT showed that neither modification effect of the treatment strategy of adopting direct or bridging MT nor interaction effect by trichotomized CBS was shown for patients with AIS regarding the overall functional disability. Despite the significantly increased rate of asymptomatic ICH in patients with CBS 7–10, other safety outcomes were not significantly different by CBS subgroups. Thereafter, our results do not support our hypothesis that the degree of clot burden alters the treatment effect of IVT. The clot burden should not alter the physician’s decision on whether to use thrombolysis or not.
We found no interaction and modification effect of IVT on the mRS distribution by stratifying thrombus burden. The previous findings showed there was no significant treatment-by-occlusion site interaction for internal carotid artery, M1, and M2.15,16 In the subgroup analysis, the stratified CBS of 0–3, 4–6, and 7–10 mostly corresponded with the occlusion site of ICA, M1, and M2, respectively. The nonsignificant treatment effect of IVT by CBS stratification may be attributed to several aspects. First, thrombus composition may also pose an important determining effect for IVT besides thrombus length.17 Second, the transfer model adopted in the DIRECT-MT is the mothership model. In the model, the working time from intravenous alteplase to groin puncture for IVT was very short, approximately 27 minutes in the DIRECT-MT, leading to inadequate time for alteplase working. Nguyen and Fischer18 also considered the treatment effect of IVT could not be reflected in the mothership paradigm but drip-and-ship model. For the latter paradigm, the time interval from needle to puncture was significantly longer, and early reperfusion was significantly increased in the drip-and-ship paradigm than in the mothership paradigm.19,20 Under the drip-and-ship paradigm, patients would potentially benefit from treatment effect of IVT, especially for distal occlusions.
The DIRECT-MT main results showed higher percentages of early reperfusion before MT in the bridging MT group but without statistical significance, and the result was similar to other randomized clinical trials.9,21,22 On the basis of our prior subgroup analysis, we found that patients with CBS 0–5 had early reperfusion more frequently when they were treated with IVT before MT.16 Likewise, for patients in the current subgroup analysis, we inferred those patients with CBS 0–3 would also benefit from early reperfusion. However, subgroup analysis showed that early reperfusion occurred more frequently in patients with CBS 4–6 in the bridging MT group, while patients with CBS 0–3 and 7–10 did not achieve this benefit. For patients with CBS 0–3, the occlusion site mostly occurred at the ICA. The proximal occlusion with large thrombus burden had poor response to IVT and could be hardly recanalized.23⇓-25 This conformed to our anticipation in the clinical practice. In the meantime, patients with CBS 4–6 had a higher rate of early reperfusion, which may be attributed to relatively short thrombus length and thrombus location of M1 segment. Arrarte Terreros et al24 also reported early recanalization mostly occurred in M1, and more often in M2 after IVT in the drip-and-ship paradigm. Moreover, we failed to observe significant change in early reperfusion in those patients with CBS 7–10 which mainly (79%) occurred at M2. As expected, treatment effect of IVT should be presented with higher recanalization rate for distal occlusions. This may be attributed to the paradigm used in DIRECT-MT. For distal occlusions, adequate time was needed for alteplase to work with the thrombus.20,23 The nonsignificant treatment effect of IVT was probably caused by limited time interval from alteplase use to groin puncture to dissolve the thrombus before MT in these patients with CBS 7–10 in the mothership paradigm.
Reperfusion is strongly associated with clinical outcomes in patients with AIS who underwent MT. A higher percentage of final successful reperfusion was observed in the bridging MT group in the main results of DIRECT-MT, though a lack of statistical significance was observed.9 Bridging MT was associated with higher rates of successful reperfusion and less thrombectomy attempts.26 In this further subgroup analysis, we found that patients with CBS 4–6 had a significantly higher rate of successful reperfusion and required less thrombectomy attempts in the bridging MT group. The occlusion site of patients with CBS 4–6 was mainly M1, and the thrombus was mostly restricted in the distal M1 or bifurcation. After IVT pretreatment, the size of thrombus was reduced, and the number of thrombectomy passes was less required to retrieve these clots.26⇓⇓-29
The main concerns about IVT pretreatment are the hemorrhagic complications. Patients with low CBS had significantly higher rates of mortality, symptomatic or asymptomatic ICH, any procedural complications, and new territory embolization than patients with high CBS. With the exception of asymptomatic ICH, other safety outcomes were comparable in CBS subgroups. Patients with CBS 7–10 had higher incidence of asymptomatic ICH in the bridging MT group, and patients with CBS 0–3 had similar safety outcomes between the two groups. The results did not support our initial assumption that IVT may have a detrimental effect, resulting in a higher rate of symptomatic ICH in patients with a large thrombus burden. In clinical practice, a large dose of unfractionated heparin is conventionally used in the direct MT group while not used in the bridging MT group. The latest evidence showed that periprocedural use of unfractionated heparin was associated with increased risk of symptomatic ICH.30 The safety outcomes could be confounded by the periprocedural use of unfractionated heparin.
There are several limitations of this subgroup analysis. First, due to post hoc analysis design with relatively small sample size and potential selection bias, the statistical analysis may be underpowered for interaction test between IVT and thrombus burden. In the meantime, the findings in the subgroup analysis were interpreted on the basis of the mothership paradigm implemented in DIRECT-MT, which cannot reflect the treatment effect of IVT in the drip-and-ship paradigm. Therefore, the result of subgroup analysis cannot be overinterpreted, and further randomized controlled trials were warranted for all paradigms.
CONCLUSIONS
Our findings of the DIRECT-MT trial did not support skipping IVT before MT based on CBS stratification due to the benefit of early reperfusion and comparable safety outcomes in the CBS subgroups. The subgroup analysis showed no modification effect of treatment strategy of using direct or bridging MT for trichotomized CBS subgroups regarding the overall disabilities. Further meta-analysis of randomized controlled trials or cohort studies are warranted to investigate the treatment effect of IVT in all paradigms.
Footnotes
Zifu Li, Yu Zhou, and Xiaoxi Zhang contributed equally to this work.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
REFERENCES
- Received July 6, 2023.
- Accepted after revision December 4, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.