
Abstract
BACKGROUND AND PURPOSE: Spontaneous intracerebral hemorrhage is a serious stroke subtype with high mortality and morbidity. Minimally invasive surgery plus thrombolysis is a promising treatment option, but it requires accurate catheter placement and real-time monitoring. The authors introduced IV flat detector CT angiography (ivFDCTA) into the minimally invasive surgery procedure for the first time, to provide vascular information and guidance for hematoma evacuation.
MATERIALS AND METHODS: Thirty-six patients with hypertensive intracerebral hemorrhage were treated with minimally invasive surgery under the guidance of ivFDCTA and flat detector CT (FDCT) in the angiography suite. The needle path and puncture depth were planned and calculated using software on the DSA workstation. The hematoma volume reduction, operation time, complications, and clinical outcomes were recorded and evaluated.
RESULTS: The mean preoperative hematoma volume of 36 patients was 35 (SD, 12) mL, the mean intraoperative volume reduction was 19 (SD, 11) mL, and the mean postoperative residual hematoma volume was 15 (SD, 8) mL. The average operation time was 59 (SD, 22) minutes. One patient had an intraoperative epidural hematoma, which improved after conservative treatment. The mean Glasgow Outcome Scale score at discharge was 4.3 (SD, 0.8), and the mean mRS score at 90 days was 2.4 (SD, 1.1).
CONCLUSIONS: The use of ivFDCTA in the evacuation of an intracerebral hemorrhage hematoma could improve the safety and efficiency of minimally invasive surgery and has shown great potential in hemorrhagic stroke management in selected patients.
ABBREVIATIONS:
- FDCT
- flat detector CT
- HICH
- hypertensive ICH
- ICH
- intracerebral hemorrhage
- ivFDCTA
- IV FDCT angiography
- MIS
- minimally invasive surgery
Spontaneous nontraumatic intracerebral hemorrhage (ICH) stroke is associated with high mortality and morbidity across the world, and hypertensive ICH (HICH) accounts for about 60%, which has become a great burden to society.1,2 Rapid expansion of the ICH and secondary bleeding are always associated with poor clinical outcome. Timely bleeding control and necessary hematoma evacuation to prevent further deterioration are the keys to critical care management of ICH. Several recent randomized studies have investigated the safety and efficacy of minimally invasive surgery (MIS) plus rtPA in patients with ICH and compared this strategy with standard medical care.3⇓-5 Although no differences were found in the primary outcome of the comparative study, a reduction in clot size to ≤15 mL was associated with better functional outcomes, suggesting the importance of effective initial hematoma removal in improved prognosis.6
Accurate catheter placement and intraoperative real-time monitoring are necessary for substantial ICH evacuation. Currently, most MIS for hematoma evacuation is guided by a stereotactic apparatus or a neurosurgical medical robot but requires additional equipment and time-consuming preparation. Recently developed mixed-reality holographic navigation technology has also demonstrated its potential in the treatment7 of ICH, but it is not widely used and has not received adequate clinical validation. Endoscopy-assisted evacuation allows hematoma evacuation under direct view; however, the puncture damage caused by craniotomy is relatively large, and the procedure needs a surgeon with greater experience and operating skills.8
Minimally invasive evacuation of ICH under the guidance of flat detector CT (FDCT) has been reported in recent years, and its safety and feasibility in intraoperative puncture guidance and real-time hematoma-evacuation monitoring have been demonstrated.9,10 In this study, we attempted to introduce IV FDCT angiography (ivFDCTA) to the treatment of HICH for the first time. A new 6-second IV DSA procedure was used, compared with previously reported FDCT-guided ICH evacuation, to implement cerebrovascular information during puncture needle path planning and to localize the hematoma. ivFDCTA is an imaging technique that enables the acquisition of the whole cerebral vasculature with a single injection of contrast media intravenously. It has been used for the visualization of intracranial artery stenosis and occlusion,11 the assessment of intracranial aneurysm,12⇓-14 and the follow-up of endovascular procedures,15⇓-17 showing its feasibility and therapeutic value in the neurology field. This study aimed to confirm the reliability of the vascular images provided by ivFDCTA for needle diameter planning and real-time guidance during ICH puncture.
MATERIALS AND METHODS
Patients
This study was approved by the ethics committee of Taicang First People’s Hospital. Patient consent for treatment was obtained according to the hospital guidelines. Between November 2020 and May 2023, thirty-six patients diagnosed with hypertensive hemorrhage were included in this study. The inclusion criteria were the following: 1) ICH with related neurologic symptoms and signs, 2) absence of cerebral hernia, 3) supratentorial ICH with a Glascow Coma Scale score of ≥9 within 72 hours of onset, and 4) a distance from the hematoma to the cortical surface of > 1 cm. The exclusion criteria were the following: 1) CTA diagnosis of secondary cerebral hemorrhage, such as aneurysm or vascular malformation, 2) mRS score of >2 before onset, and 3) long-term use of aspirin or anticoagulant drugs.
All patients underwent cranial CT (Somatom go.Fit; Siemens) before the hematoma evacuation. The volumes of the hematoma and surrounding edema were calculated by 3 separate radiologists in a single-blind way, and the average value was adopted. The volume of the hematoma (milliliters) = Length of the Maximal Hematoma Layer × Width of the Maximal Hematoma Layer × Number of Hematoma Layers × π/6.
ivFDCTA
Patients were placed in a supine position under local anesthesia. Images were acquired using a 16-bit Artis Q ceiling angiography system (Siemens) with the patient in a supine position. All patients received general anesthesia to ensure coordination and image quality. ivFDCTA was acquired by using a manually triggered 6-second DSA DynaCT Head program, which includes a native and contrast-enhanced sweep. The contrast-enhanced run was not started until contrast media was seen in the intracranial ICA C1–C2 during the bolus-watching phase. Seventy milliliters of iodinated contrast media (320 mg/mL, Yangtze River Pharmaceutical Group) was injected into a cubital vein at a pressure of 300 psi through a 20F angiocatheter (BD Intima II Plus; Becton, Dickinson and Company) at a flow rate of 5 mL/s using a power injector. The acquisition of a native image was started after the beginning of contrast injection. Data acquisition per run was performed with the following parameters: acquisition time, 6 seconds per run; tube voltage, 70 kV; section matrix, 512 × 512; flat detector size, 30 × 40 cm; total rotation angle, 200°; angulation step, 0.5° per frame; 397 frames per run; dose, 1.2 µGy/fr. Window center and width of the bolus check sequence were set at 130 and 2500, respectively. Contrast-enhanced images were viewed in cross-sectional MIP thin mode, with a section thickness of 2 mm.
Needle Path Planning and Puncture Guidance
Native and contrast-enhanced images acquired by ivFDCTA were viewed in DualVolume mode (Siemens). The opacity of each volume was adjusted to enable a clear display of both the intracranial hematoma and vessels. Needle path and puncture depth were planned and calculated using the software syngo Needle Guidance on the DSA workstation (syngo X-Workplace; Siemens). The target point was chosen by selecting a point within the hematoma 1 cm away from the boundaries of the hematoma. The entry point was chosen on either side of the temporal site that was close to the hematoma. The needle guidance software enables a preview of the puncture path from the entry point to the target from 3 cross-sectional perspectives (sagittal, coronal, and axial). To prevent unintentional bleeding, we could adjust the planning path if there is the potential for a large blood vessel to be punctured (Fig 1).

Needle path planning and puncture guidance on the ivFDCTA image using syngo Needle Guidance software. Hemorrhage in the left basal ganglia. A puncture needle path was planned by defining the skull entry point and hematoma target point. The final puncture entry point (B) was adjusted to 1 cm before the first planning (A) to avoid the intracranial vascular cluster at the temporal side (red arrow).
Hematoma Evacuation and Intraoperative Monitoring
Once the needle path was determined, a corresponding C-arm working angle in bull’s eye view was sent to the C-arm, and a red laser crosshair was displayed on patient’s head to indicate the puncture entry point.
Minimally invasive craniopuncture was performed using a YL-1 Needle (Beijing WanTeFu Medical Apparatus). The YL-1 needle, with a diameter of 3 mm, is an internal drilling needle that is enclosed by a casing with small holes at the end to facilitate fluid flow. Initially, an electric drill is used in conjunction with the YL-1 needle for puncturing purposes. The first FDCT scan is performed when the puncture needle is fixed to the skull and the dura is not punctured. According to the results of FDCT, the direction of puncture is adjusted and the dural puncture is continued. To reach the center of the hematoma, we removed the assembly comprising the internal drill needle. To minimize potential brain damage risks, we used plastic needles as substitutes for internal drilling needles. These plastic needles have a blunt end and are 2 mm longer than their internal drill counterparts. The puncture needle is drilled through the skull and into the hematoma before the cannula is fixed to the skull and the hematoma is aspirated. A 20-second DynaCT scan (Siemens) was performed as necessary to monitor the degree of aspiration.
For patients with a large hematoma volume, it is often difficult to achieve a satisfactory hematoma-removal effect with 1 puncture aspiration. FDCT in the operation enables the surgeon to monitor the situation in real-time and perform a second puncture under sterile conditions if necessary (Fig 2). Aspiration was stopped when the hematoma volume was reduced by two-thirds or was <15 mL, shown in the FDCT image.

Monitoring of intraoperative hematoma evacuation under FDCT. The patient had an estimated hematoma volume of 45 mL. A, Discharge of 10 mL from the first hematoma. B, Laser crosshair indicated the second puncture entry point. C, A second puncture was performed, and the needle position was confirmed under FDCT. A total estimated volume of 25 mL of hematoma was aspirated. D, Postoperative CT shows a residual hematoma of 10 mL.
The whole procedure is summarized in a flow chart shown in Fig 3.

Flow chart of the ivFDCTA- and FDCT-guided HICH evacuation.
Surgery Evaluation
Following initial aspiration, a lysis fluid-containing urokinase is injected to facilitate further aspiration. The thrombolytic agent is reintroduced into the hematoma every 6–12 hours. A follow-up CT scan is performed 1–3 days after the initial drainage to measure the amount of blood remaining. The drainage needle remains in the brain for 3–5 days.
Common postoperative complications were recorded during hospitalization, including postoperative rebleeding, intracranial infection, and gastrointestinal bleeding.
Statistical Analysis
All data were analyzed by SPSS software, Version 16.0 (IBM). The data were presented as mean (SD).
RESULTS
Thirty-six patients were included in this study. The mean preoperative hematoma volume of 36 patients was 35 (SD, 12) mL, the mean intraoperative volume reduction was 19 (SD, 11) mL, and the mean postoperative residual hematoma volume was 15 (SD, 8) mL. The average operation time was 59 (SD, 22) minutes, there was an intraoperative epidural hematoma in 1 case, and the hematoma volume was 3 mL, which improved after conservative treatment. The maximum and minimum positioning errors were 3.5 and 0.3 mm. Patients’ basic characteristics and postoperative evaluation are listed in the Table.
| Characteristics | |
|---|---|
| Age (mean) (yr) | 53 (SD, 12) |
| Sex (male) (%) | 81% |
| NIHSS score on admission (median) | 17 (SD, 6) |
| Preoperative GCS score (mean) | 10 (SD, 2) |
| GOS | 4.3 (SD, 0.8) |
| 90-Day mRS | 2.4 (SD, 1.1) |
| Complications | 2.7% |
| Days to discharge | 16.4 (SD, 5.3) |
Note:—GCS indicates Glasgow Coma Scale; GOS, Glasgow Outcome Score.
Basic characteristics and postoperative evaluation of all 36 patients
DISCUSSION
ICH accounts for 10%–40% of all strokes worldwide and is as high as 40% in Asia. The fatality and disability rate exceeds 60%, and the incidence is increasing year by year. Possible treatments of ICH include1 conservative medical treatment for hemostasis and coagulopathy or2 surgical treatment to remove the hematoma. Whether surgery can improve the prognosis of patients with ICH remains controversial. The Surgical Treatment for Ischemic Heart Failure (STICH) and STICH II trials aimed to investigate the effectiveness of early surgery (mostly craniotomy) compared with initial medical treatment alone, and the results were neutral. However, the question about the performance of less invasive surgery to remove ICH was raised. The randomized controlled Minimally Invasive Surgery Plus Rt-PA for ICH Evacuation (MISTIE)4 II study demonstrated the safety and efficacy of alteplase in combination with MIS in ICH management. The MISTIE III trial compared the image-guided MISTIE treatment with standard medical care, but no improvement was found in the functional outcome at 365 days.5 However, in the subgroup study in which ICH volume was reduced to ≤15 mL or was >70%, better mRS scores could be achieved. This finding indicates the importance of surgery efficiency in determining good functional outcome of MIS in ICH evacuation.6
The effectiveness of hematoma evacuation is heavily dependent on the decreased hematoma volume. According to our experience, the hematoma may contain a mixture of liquid, semisolid, and solid material throughout the evacuation procedure, making it impossible to reduce the volume equally. Accurate catheter placement with as much contact area as possible with the hematoma and intraoperative real-time monitoring are essential to ensure the safety and effectiveness of hematoma evacuation and avoid unintentional loss of brain tissue. The angiography system with intraoperative FDCT imaging of the brain parenchyma to assess the degree of ICH evacuation has been described before, and the needle guidance software enables precise catheter placement and navigation accuracy, in which puncture path planning is realized on intraoperative FDCT 3D volume images by identifying the target hematoma and the entry point on the skull. A virtual flight along the needle path can be checked in 3 MPR (Multiplanar Reformation) segments to verify that the needle path does not injure any anatomic structure, and the laser positioner light is automatically on and indicates the entry point on the skull.9,10,18
Minimally invasive craniopuncture using a YL-1 needle via a temporal approach has become a standard surgical method commonly used in China. It has shown the advantages of a small deviation, low cost, and low surgical difficulty with good functional outcomes through multiple randomized clinical trials, making it a practical and promising technique for ICH clot removal, especially in primary hospitals with large patient populations.19⇓⇓-22 Compared with conventional CT-guided stereotactic aspiration, craniopuncture under the guidance of FDCT in an interventional operating room has become more suitable due to better environment hygiene and emergency event responses. However, it can be challenging to securely avoid the external carotid artery and major vessels of the lateral fissure when using a temporal approach. Prior research did not include cerebral vascular information in craniopuncture; the authors used noncontrast FDCT solely for planning and guidance.9,10,18
In this study, we first introduced ivFDCTA into the hematoma-evacuation workflow. All the arteries of the brain can be seen due to the IV-injection acquisition protocol, which could be used for puncture needle path planning to prevent secondary bleeding. In previous studies, the rebleeding rate of minimally invasive brain puncture under CT was 8.8% to 10%.23 Chen et al24 reported a study of 48 patients with ICH treated with the YL-1 needle under CT guidance; 2 of these cases required repositioning the puncture needle due to inadequate initial placement. Three (6.3%) patients experienced early re-bleeding within the first 3 postoperative days, a rate higher than in our study. The 6-second ivFDCTA protocol is substantially faster than the 20-second previously reported protocol, but it provides adequate image quality for hematoma identification, reducing the radiation exposure and accelerating the preparation for the procedure. As shown in Fig 1, during puncture planning, both blood vessels and hematoma could be observed by displaying the ivFDCTA native and contrast-enhanced images, allowing the physician to plan the needle path safely and more accurately to avoid large vessels and reduce intraoperative bleeding and complications. In case of a large hematoma, it may be difficult to achieve the target of volume reduction with a single puncture, and multiple target points may be needed.25 Marquardt et al26 demonstrated the safety and efficiency of multiple target aspiration techniques. Zhou et al20 compared 80 patients with HICH who received CT-guided MIS and showed that the clearance rate of hematomas in patients with hematomas of >40 mL with a single puncture was less than in those with multiple punctures. With the ivFDCTA in ICH removal, the large vessels on the puncture tract can be accurately visualized and located, and intraoperative CT enables multiple punctures performed safely and sterilely in the interventional operating room (Fig 2).
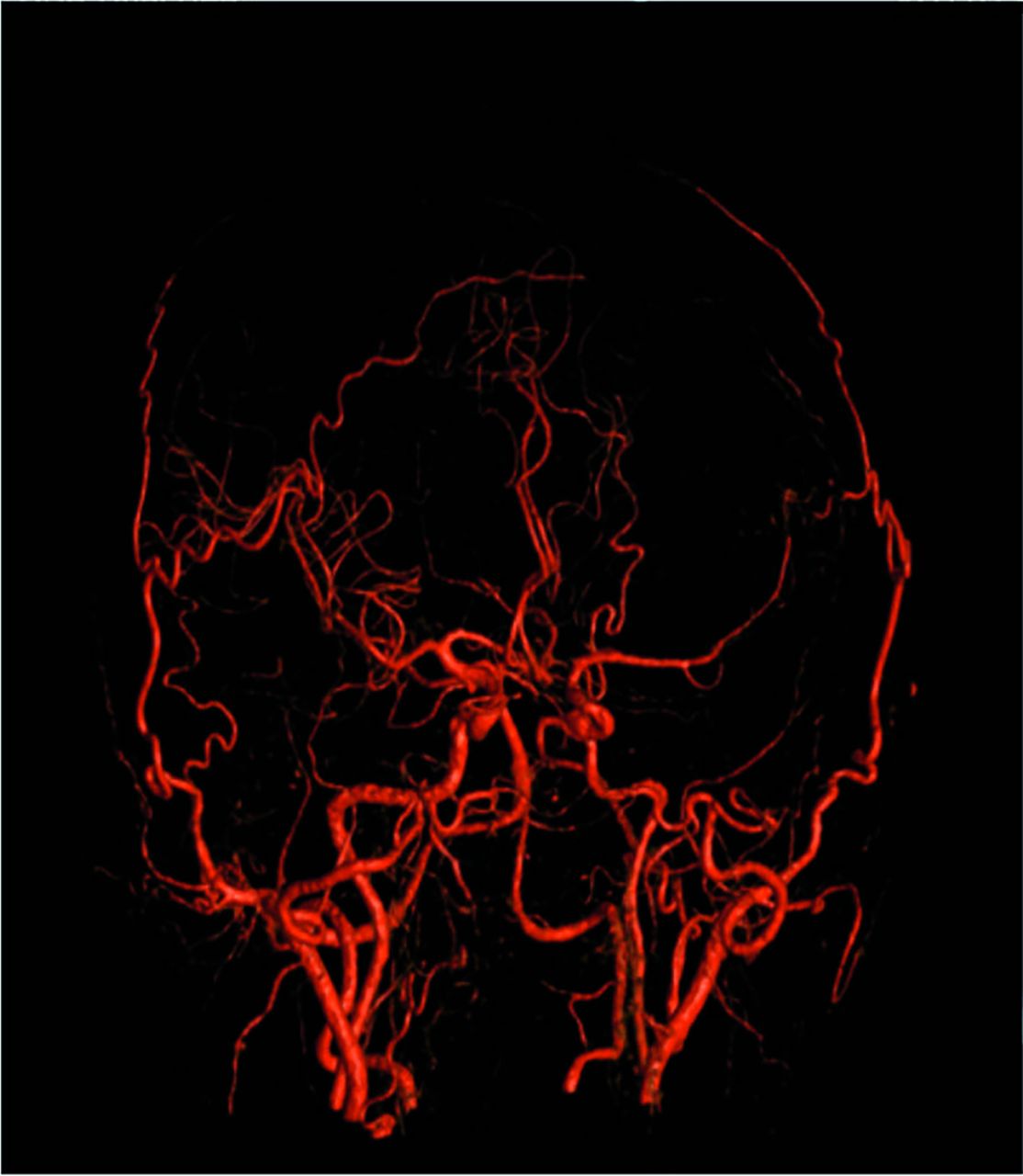
Because it is reliable and convenient, minimally invasive puncture has been widely used in China to treat HICH. The 2 most commonly used puncture needles are the soft tube, also called the “soft channel” approach, and the YL-1 puncture needle, also known as the “hard-channel” technique. Comparisons between the 2 methods are rare, yet available. In a study involving 150 patients, Xia et al22 found that there was no discernible difference in the amount of hematoma and perihematomal edema on day 7 between the 2 techniques. The benefits of the soft tube tend to be ease of direction adjustment and quick rinsing. We chose the hard channel because it allows us to fully use intraoperative FDCT while enabling safe adjustments outside the dura and accurate placement at the assigned position using the skull-fixation technique. If the first puncture volume reduction is not satisfactory, multiple punctures can be performed in a sterile state. On the contrary, due to the presence of the C-arm, the operating space directly above the head during soft-channel puncture will be affected.ivFDCTA is a technique to generate CTA-like images using DSA through noninvasive IV contrast media injection. In the field of neurology, this technique was first proposed as a noninvasive alternative for follow-up after placement of intracranial devices such as stents and flow diverters and enabled good visualization of both the device and vessel lumen.15⇓-17 ivFDCTA also shows comparable image quality with 2D and 3D DSA in delineating and diagnosing vessel stenosis and aneurysms, and even better quality in visualizing complex aneurysms.12⇓-14 In the ICH evacuation procedure, we also found that ivFDCTA has the potential to be used for a rapid screening of the cerebral vasculature malformations to avoid secondary bleeding during the evacuation procedure. According to the guideline for ICH management, CTA is recommended for detection of some structural causes of secondary ICH and signs of hematoma expansion.27 However, patients with ICH, especially in those with a high NHISS score, often have severe agitation and require sedation to undergo a CTA scan. Nevertheless, a standard anesthesia procedure and care management are not available due to limited space and equipment resources in the CT room. Most CT examination rooms lack sufficient first aid and patient-monitoring equipment to handle emergencies, and patient risks may increase during suite transfers. Furthermore, bone artifacts and spatial resolution may restrict the precision of CTA-based vascular malformation diagnosis and geometric delineation. In addition to generating 2D cross-sectional images, the ivFDCTA methodology we describe in this article could also generate IV 3D DSA (Fig 4), which provides a volumetric view of the cerebral arteries and enables determination of the optimal C-arm working angle if intraoperative endovascular treatment is necessary. Therefore, with the use of ivFDCTA, clinical steps including screening for cerebrovascular disease, puncture needle path planning and navigation, hematoma evacuation, and endovascular treatment could all be performed in the angiography suite. This one-stop cerebral hemorrhage management workflow has the potential to eliminate the treatment delays and risks during transfer and increase the safety of the procedure and the efficiency of hematoma evacuation.

IV 3D DSA image.
Our study has limitations. First, this is a retrospective single-center study. The amount of patient data collected is small and requires further research and the completion of statistical analyses of long-term neurologic outcomes. Second, there is no comparison group in this study. Comparison between FDCT and ivFDCTA guidance will be included to further explore the clinical value of ivFDCT in ICH management. Third, the initial calculation of the hematoma volume according to the Tada formula (Hematoma Amount = Long Diameter of the Largest Level of Hematoma × Short Diameter of the Largest Level of Hematoma × Number of Levels of Hematoma × π/6) is based on the principle that the bleeding focus is assumed to be an elliptic sphere, which has evolved from the formula for calculating the volume of an elliptic sphere. For the irregular shape of a hematoma, the calculation error is large and the calculated volume is often larger than the actual volume of the hematoma. Another more accurate hematoma calculation method needs to be adopted.
CONCLUSIONS
Cerebral hemorrhage is still a fatal condition. It is necessary to continue improving the treatment of ICH for better clinical outcomes. In this study, for the first time, we introduced the application of ivFDCTA in the treatment of HICH MIS treatment and demonstrated its safety and feasibility. The use of ivFDCTA in ICH hematoma evacuation could improve the safety of MIS and has shown great potential in hemorrhagic stroke management in selected patients.
Footnotes
Z. Shu and W. Wang are co-first authors.
This work was supported by the Taicang First People’s Hospital Specific Project Fund. TCYY2020YJKT07.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received October 30, 2023.
- Accepted after revision January 11, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.