
Abstract
SUMMARY: Pediatric large-vessel occlusion has a poor natural history. Recent retrospective studies have demonstrated the potential benefits, feasibility, and safety profile of mechanical thrombectomy in children. However, the role of thrombectomy in pediatric M2 occlusions remains uncertain. In this clinical report, we present a multicenter series of 6 pediatric patients with acute M2 occlusion (female = 1, male = 5; age range, 0.9–16.0 years, mean = 9.2). All 6 patients having undergone thrombectomy had excellent clinical outcomes (pediatric mRS = 0–1) at 3 months and final available follow-up (median, 12 months; range, 3–72 months). Factors relevant to treatment decision-making in pediatric M2 occlusions are discussed, including the important role of multidisciplinary team discussions during acute management.
ABBREVIATIONS:
- LVO
- large-vessel occlusion
- MeVO
- medium-vessel occlusion
- mTICI
- modified treatment in cerebral ischemia
- ped-mRS
- pediatric mRS
- Ped-NIHSS
- pediatric NIHSS
Pediatric ischemic stroke due to large-vessel occlusion (LVO) has a poor natural history.1 Approximately three-quarters of patients managed conservatively have moderate-to-severe disability or death at 3 months after stroke onset.1 Given these poor outcomes and the clear benefit of mechanical thrombectomy in adults,2 mechanical thrombectomy is increasingly used in pediatric LVO stroke despite a lack of randomized trial evidence in children.
A recent retrospective case-control study demonstrated improved clinical outcomes in 26 children who received mechanical thrombectomy (intracranial ICA = 10, M1 = 11, M2 = 3, basilar = 2) compared with 26 matched controls with acute LVO ischemic stroke.3 Favorable outcomes were also identified from the multicenter retrospective Save ChildS cohort study (median mRS score = 1.0).4 These results suggest that mechanical thrombectomy is beneficial for selected pediatric patients with LVO.
In adults, there is increasing interest in the treatment of medium-vessel occlusion (MeVO) using mechanical thrombectomy, particularly for the second segment (M2) of the MCA.5 Subgroup analysis of a large prospective registry for mechanical thrombectomy in adults demonstrated favorable clinical outcomes (mRS = 0–2 at 90 days) in 72.5% of patients with M2 occlusion.6 There are multiple randomized trials underway comparing thrombectomy with the best medical management for MeVO in adults.
The role of mechanical thrombectomy for acute M2 occlusion in children is uncertain. Current clinical guidelines provide no recommendations regarding thrombectomy for pediatric MeVO.7 However, depending on patient-specific neurovascular anatomy and the location of the occlusion (dominant-versus-nondominant hemisphere, perirolandic-versus-opercular branches), M2 segment occlusions can be as disabling as some M1 segment occlusions.5,8
In this study, we present the clinical outcomes from 6 pediatric patients with M2 segment occlusion treated with mechanical thrombectomy, forming the largest published series in the literature, to the best of our knowledge.
Case Series
Institutional ethics approval was granted at each center. This was a retrospective, multicenter cohort study involving 3 tertiary pediatric hospitals and 1 adult hospital with the capability of providing mechanical thrombectomy for adolescents across New South Wales, Australia, and Ontario, Canada. Stroke registry databases were queried from January 2015 to August 2023 for all patients younger than 18 years of age with radiologically confirmed acute M2 occlusion (using CTA, MRA, or DSA) who were treated with mechanical thrombectomy. De-identified data were then pooled for analysis. Clinical outcomes were assessed using the pediatric modification of the mRS (ped-mRS)9 score at 3 months following stroke onset and at final available follow-up.
All available cases were included. Six consecutive pediatric patients with M2 occlusion who received mechanical thrombectomy were identified (female = 1, male = 5; age range, 0.9–16.0 years; mean = 9.2; SD = 6.60) (On-line Supplemental Data). Two patients also received bridging IV thrombolysis without clinical improvement before commencing thrombectomy. Three of the 6 patients having undergone thrombectomy were also included in our previously published case-control study.3 Four of the 6 patients had known congenital heart disease, and a fifth patient was found to have a patent foramen ovale with positive findings on a bubble test echocardiogram after the stroke episode. None of the patients had a prior history of stroke or recurrent stroke during the follow-up period. None of the patients had diagnosed developmental delay before their stroke episodes.
The decision to offer mechanical thrombectomy was undertaken on a case-by-case basis following multidisciplinary discussions between pediatric neurology and pediatric interventional neuroradiology colleagues. None of the sites involved had specific guidelines for the treatment of M2 occlusion in pediatric patients due to the rarity of the condition and sparsity of data on the subject in the literature. Clinical and imaging factors considered relevant during treatment decision-making are detailed in the discussion.
All 6 patients had successful angiographic recanalization (modified treatment in cerebral ischemia [mTICI] = 2b–3) and no symptoms or functional disabilities (defined as excellent outcome; ped-mRS 0–110) at 3 months poststroke as well as at the final available follow-up (mean = 14 months) (Online Supplemental Data). The mean pediatric NIHSS (Ped-NIHSS) score at baseline was 8.5 ([SD, 3.73]; range, 3–13), and 24 hours postprocedure, it was 1.7 ([SD, 1.4]; range, 0–3; mean reduction = 6.8 [SD, 2.7]; range, 3–10).
No patients developed symptomatic intracranial hemorrhage or required decompressive craniectomy. One patient who was on anticoagulation had an asymptomatic SAH in the ipsilateral Sylvian fissure on CT at 24 hours and developed a delayed femoral artery pseudoaneurysm successfully managed with percutaneous thrombin injection. Two patients having undergone thrombectomy had intraprocedural angiographic vasospasm following stent-retrieval use, successfully treated with intra-arterial verapamil injection in both cases (Fig 1).

Oblique anterior-posterior-projection DSA images with a right ICA injection during a mechanical thrombectomy procedure. An 11-month-old infant (patient 4 in the Online Supplemental Data) with congenital cardiac disease had reduced movement of the left upper limb and face after waking from a nap. CTA demonstrated a right MCA proximal M2 occlusion. A, Subocclusive thrombus involving the proximal aspect of the right MCA superior M2 division (white arrow). B, Following a single-pass mechanical thrombectomy with a 3-mm-diameter stent retriever, angiographic vasospasm was present in the recanalized vessel segment (white arrow). C, Vasospasm resolution was noted after intra-arterial infusion of verapamil (1.5 mg) via the right ICA 4F catheter. The ped-mRS score at 3 months was 1.
Case Example.
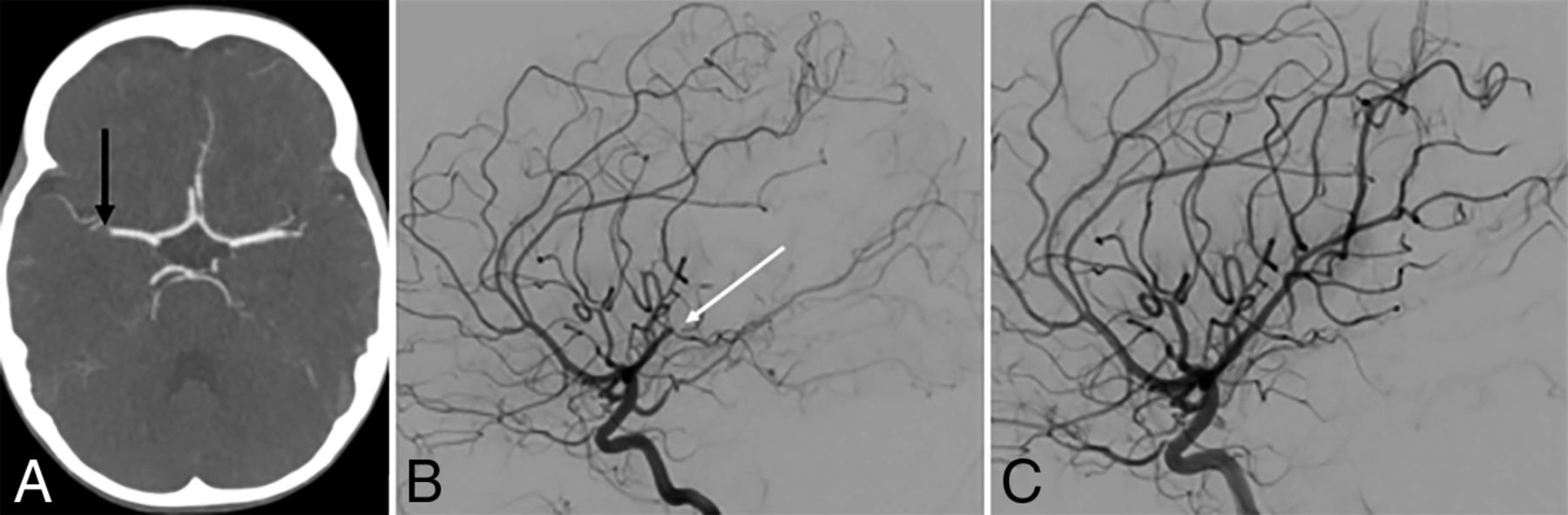
Patient 3 in our series (Online Supplemental Data) illustrates successful use of thrombectomy for a 3-year-old boy with a low and fluctuating Ped-NIHSS score. DSA demonstrated occlusion of the nondominant hemisphere perirolandic M2 division after initial CTA demonstrated a distal M1 occlusion (Fig 2). While it could be argued that this case should be managed conservatively, during the multidisciplinary discussion, the potential long-term impact of a perirolandic infarct was considered highly detrimental compared with the risks of proceeding with the intervention.5,8 Mechanical thrombectomy was successfully performed using stent retrieval combined with distal aspiration, achieving an mTICI 3 recanalization. The patient was completely asymptomatic at 3- and 12-month follow-ups (ped-mRS = 0).

A 3-year-old patient (patient 3 in the Online Supplemental Data) developed fluctuating weakness of the left upper limb (Ped-NIHSS 3) after recent cardiac surgery for cor triatriatum. A, Axial CT angiogram demonstrates a filling defect in the right MCA distal M1 segment (black arrow). B, Lateral-projection DSA image with a right ICA injection demonstrates interval migration of the thrombus to the right MCA posterior (perirolandic) mid-M2 division (white arrow). After multidisciplinary discussion regarding the potential long-term disabling impact of a perirolandic infarct, it was agreed to proceed to the mechanical thrombectomy. C, After 2 passes with a 3-mm-diameter stent retriever, there was successful recanalization of the right perirolandic posterior M2 division. The ped-mRS score at 3 months was 0.
DISCUSSION
In this case series, we demonstrated successful use of mechanical thrombectomy in 6 pediatric patients with M2 occlusion. All 6 patients had excellent clinical outcomes (ped-mRS = 0–1) at 3 months poststroke and final follow-up. While the sample sizes are too small for meaningful comparative statistical testing, the 5 pediatric patients with M2 occlusion managed with best medical treatment alone from our previously published case-control study all had mild-to-moderately severe disability at 3 months poststroke (ped-mRS = 2–4).3
No patients developed symptomatic intracranial hemorrhage or required decompressive craniectomy. The procedural complications (detailed above) were all minor with no long-term sequelae. In our view, postretrieval vasospasm in young children should be anticipated, and antispasmodic medications should be drawn up and ready for intra-arterial infusion. Overall, MeVO thrombectomy in this small pediatric sample appears relatively safe.
Close collaboration between pediatric neurology and interventional neuroradiology colleagues is essential for appropriate patient selection. During multidisciplinary team discussions for pediatric M2 occlusions, one should consider the following points:
1) Patient age and premorbid clinical status
2) Ped-NIHSS score
3) Probable stroke etiology
4) Nondominant-versus-dominant hemisphere involvement
5) Opercular-versus-perirolandic cortical involvement5
6) Presence of speech or dominant hand impairment
7) Overall risk profile of thrombectomy tailored to the individual patient
8)Availability of pediatric stroke and neurointerventional expertise.
Patients with suspected focal cerebral arteriopathy or possible Moyamoya syndrome should be considered carefully, with a bias toward medical therapy alone.7 The informed consent process undertaken with the patients’ caregivers must be tailored on the basis of the above information, and the balance of risks versus benefits should be clearly communicated.
We would argue against using the Ped-NIHSS score in isolation for treatment decisions. Delayed deterioration of patients with LVO presenting with lower NIHSS scores is described in both pediatric11 and adult settings.12 Collateral blood flow within regions of the penumbra can fluctuate with time, and deterioration of such flow results in delayed infarct growth.13 Therefore, the condition of the child with a fluctuating Ped-NIHSS score may deteriorate during periods of relative hypotension (such as sleep), with a potential loss of treatment options. Interrater reliability of the Ped-NIHSS is lower when testing sensory/visual domains and is not validated in children younger than 2 years of age.14 Therefore, the Ped-NIHSS score should be considered in the wider context of clinical presentation, occlusion location, and potential long-term disability during a longer life span.
The role of perfusion imaging for the treatment decision-making in pediatric LVO stroke remains uncertain. Existing pediatric stroke guidelines make no recommendations regarding the use of CT perfusion or MR perfusion imaging for patient selection.7,15 Quantitative parameters on CT perfusion imaging are known to vary with age during childhood, and this aspect must be considered during interpretation.16 Recent evidence suggests that performing perfusion imaging does not delay the time to recanalization in children treated with mechanical thrombectomy, that target mismatch criteria do not correlate with functional outcome, but a favorable hypoperfusion intensity ratio does correlate with clinical outcomes.17 In our experience, perfusion imaging can be helpful in borderline cases but is not sufficient to exclude a patient from being offered thrombectomy.
Our study has several limitations. First, the sample size is small but does form the largest published series of pediatric patients with M2 occlusion treated with thrombectomy. Second, there is probable underlying selection bias when selecting pediatric patients for thrombectomy in this context. This can be seen in the significantly greater delays in acquiring imaging in the control group from our previously published case-control study.3 Third, the role of thrombectomy for M2 occlusions in adults is still being assessed by at least 3 randomized trials. Fourth, 1 patient having undergone thrombectomy (case 4) was 11 months of age. The role of thrombectomy in infants remains controversial. Fifth, the main stroke etiologies in our study were cardioembolism and dissection. Pediatric stroke is heterogeneous, precluding generalization to the broader pediatric stroke population. Finally, the ped-mRS is potentially biased toward motor outcomes.
CONCLUSIONS
Mechanical thrombectomy for children with acute M2 occlusion is feasible, with a reasonable risk-benefit profile when appropriately selected by multidisciplinary care teams with expertise in pediatric stroke.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received October 6, 2023.
- Accepted after revision January 8, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.