
Abstract
SUMMARY: We report the serial MR findings and histologic features of intracerebral xanthoma in a patient with hyperlipidemia. MR imaging revealed nodule formations with variable degrees of edema and enhancement in the perivascular spaces. In some lesions, high-signal-intensity foci were observed on unenhanced T1-weighted images, which suggest lipid contents of the lesion.
Xanthomas are soft tissue tumors composed of lipid-laden foam cells, which are histiocytes containing cytoplasmic lipid material. They usually occur in patients with pathologic levels of serum lipid. The nidus of xanthoma formation is often a site of local trauma; therefore, the most common site of xanthomas are superficially exposed skin and tendons.1 Intracranial xanthomas are extremely rare, and, when present, they are usually extra-axial.2–4
We describe a case of intracerebral xanthoma occurring in a 55-year-old woman with follow-up results during a 15-month period.
Case Report
A 55-year-old woman presented with a 1-month history of headache and blurred vision. Neuro-ophthalmologic examination revealed left homonymous hemianopsia. Her blood biochemistry findings were notable for hyperlipidemia at admission: cholesterol 287 mg/dL (normal range, 130–240 mg/dL), triglyceride 269 mg/dL (normal range, 30–200 mg/dL), low-density lipoprotein cholesterol 190 mg/dL (normal, <120 mg/dL).
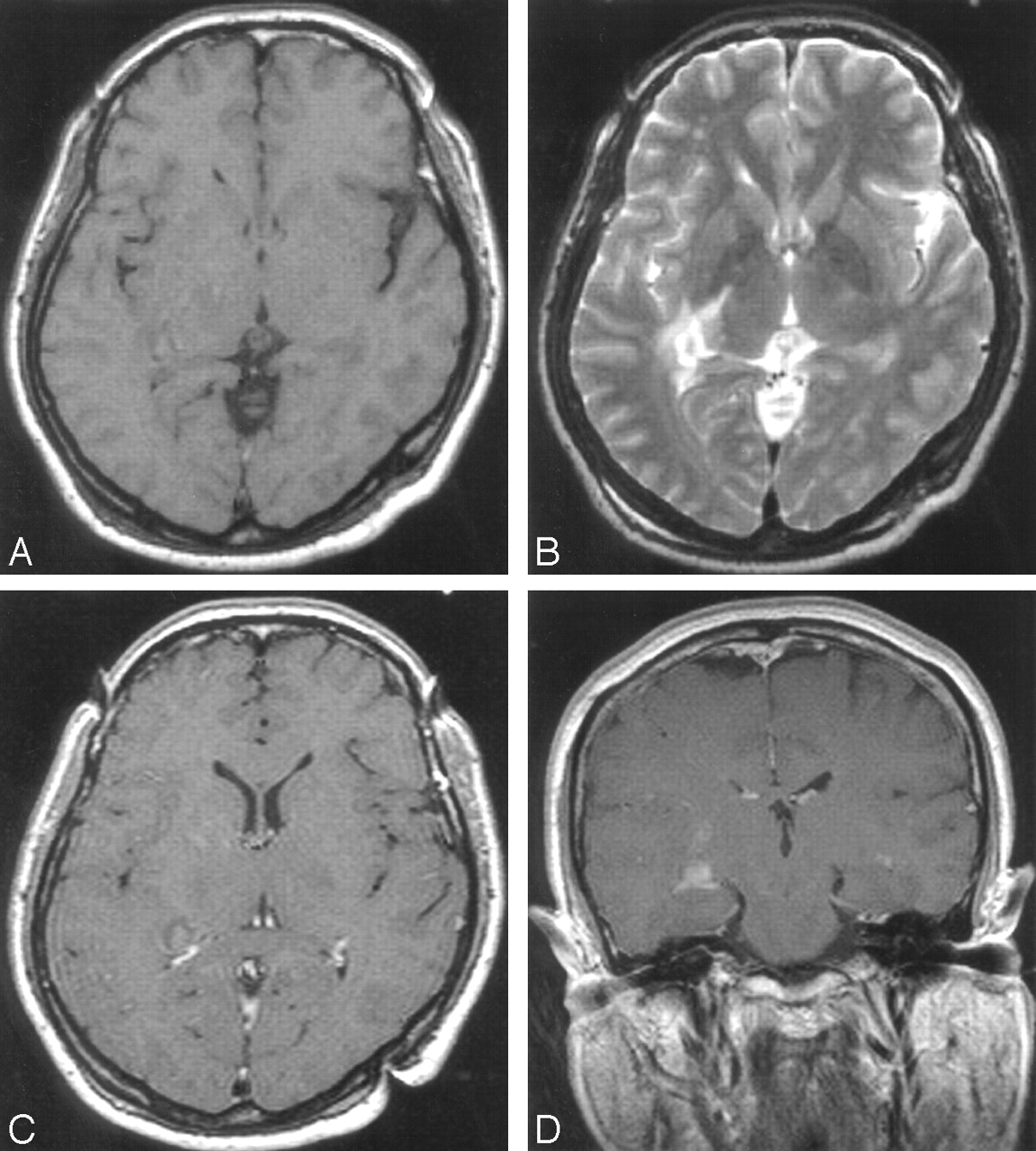
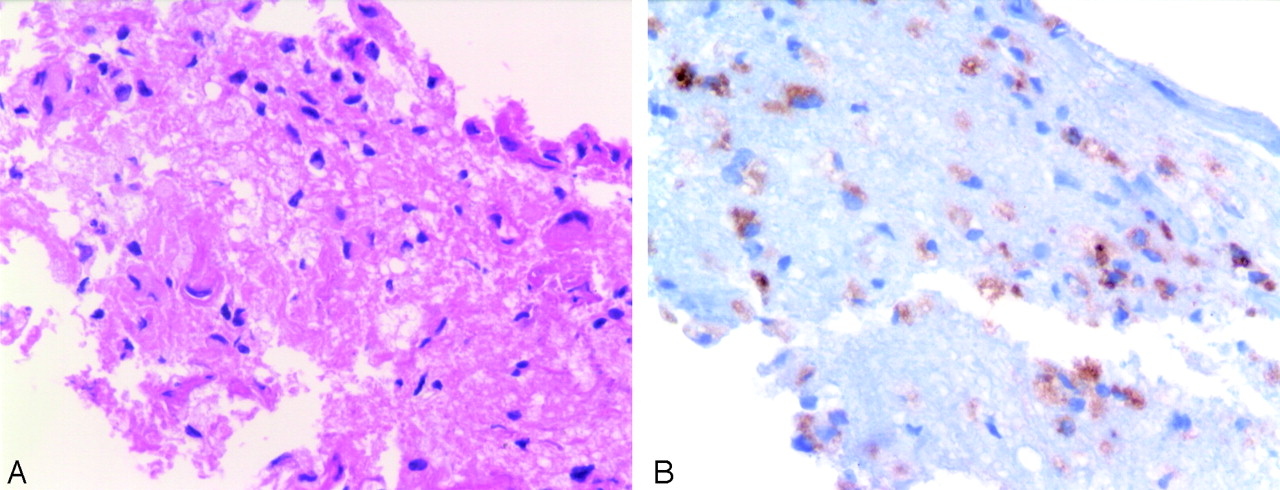
MR images revealed focal mass with vasogenic edema in the periventricular white matter near the right temporal horn. The lesion showed low signal intensity on T1-weighted images (Fig 1A) and high signal intensity on T2-weighted images (Fig 1B). In the center of the lesion, iso- to high-signal-intensity focus was seen on T1-weighted images, and the signal intensity of this focus was low on T2-weighted images. Gadolinium-enhanced T1-weighted images showed strong enhancement in the center of the lesion and subtle peripheral enhancement (Figs 1C, -D). A primary brain tumor such as lymphoma or glioma was considered, and a stereotactic biopsy was performed. On histologic examination, the lesion was composed of sheets of foamy cells with abundant vacuolated cytoplasm. The infiltrating foamy cells exhibited positive reaction for CD68, a panhistiocytic marker, but negative reactions for CD1a and S-100 protein. Findings were consistent with the histiocytic nature of the lesion. The lack of S-100 protein and CD1a reactivity made it possible to rule out the diagnosis of Langerhans cell histiocytosis. The foamy cells were also negative for GFAP, a glial marker, which ruled out the possibility of lipidized low-grade glioma (Fig 2). On the basis of these results, a conclusive diagnosis of xanthoma was established. The patient was treated with administration of a low dose of dexamethasone(4 mmg/day for 7 days, 2 mmg/day for 3 days, and 1 mmg/day for 2 days).

Initial MR imaging before stereotactic biopsy. Right temporal periventricular mass lesion is seen on T1-weighted (A), T2-weighted (B), and contrast-enhanced T1-weighted images (C and D).

Histologic findings. A, Abundant foamy histiocytes infiltrated in glial parenchyma (H&E, ×400). B, Most infiltrating cells show immunoreactivity for CD68 with intense cytoplasmic pattern (×400).
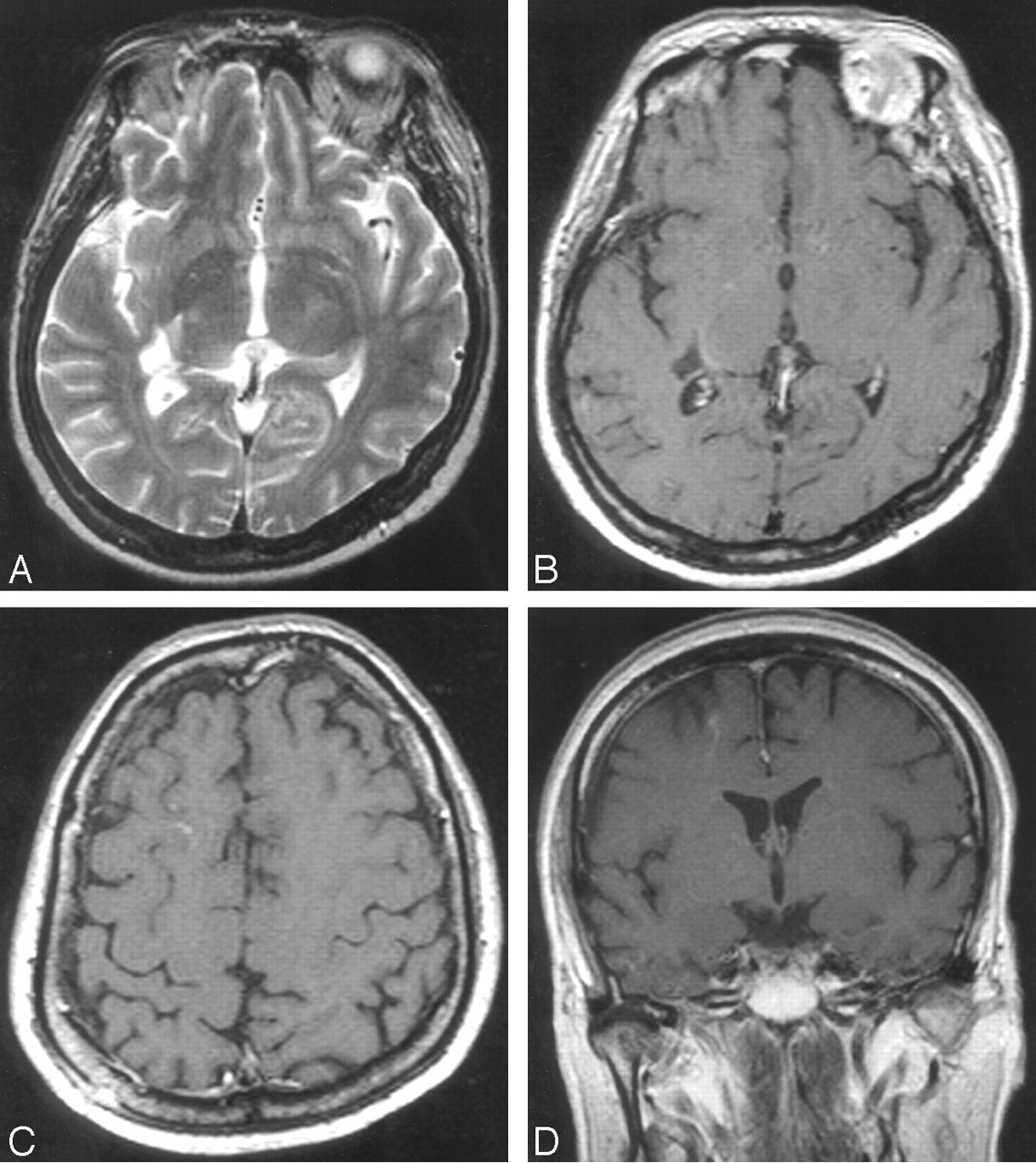
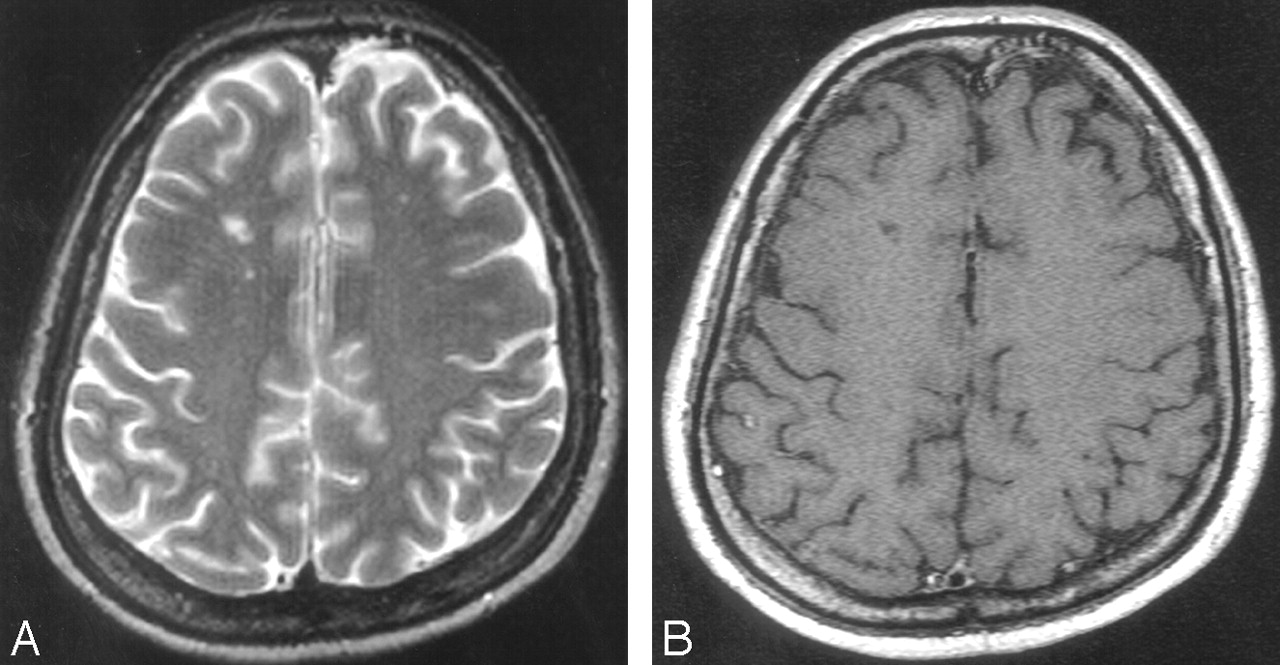
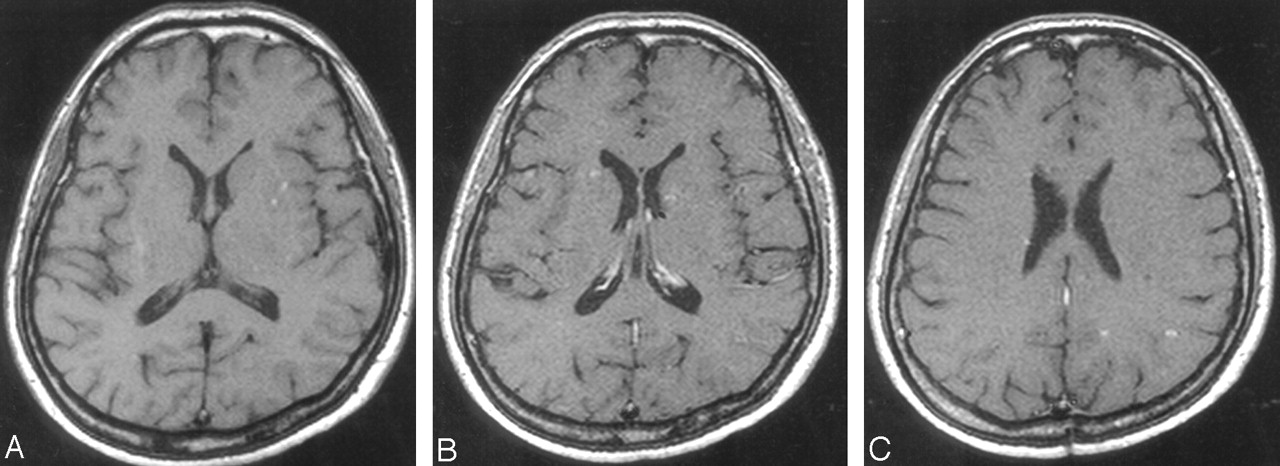
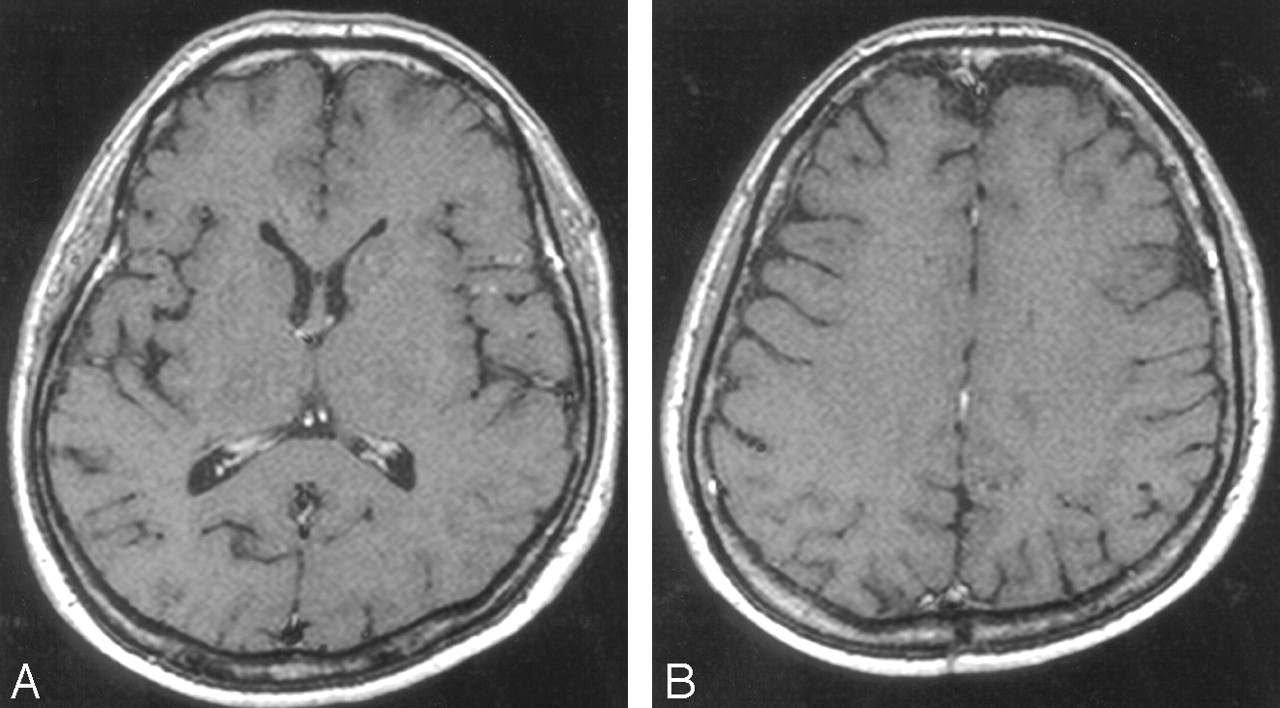
Serial MR imaging was performed during a 15-month period. One-month follow-up MR imaging showed complete resolution of the periventricular lesion with residual focal malactic cavity (Figs 3A, -B), but a new lesion developed in the right frontal lobe. This lesion showed low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, and irregular nodular and linear enhancement was observed without significant mass effect or edema on contrast-enhanced T1-weighted images (Figs 3C, -D). We presumed this lesion to be a new xanthomatous lesion, but the findings were nonspecific. At that time, the patient’s symptoms improved and the physician decided to observe without treatment. The right frontal lesion also resolved, and a residual focal malacic change was seen on the 4-month follow-up images (Fig 4). At 1-year follow-up, T1-weighted images showed characteristic multiple high-signal-intensity areas in both basal ganglia (Fig 5A). Contrast-enhanced T1-weighted images also showed focal enhancement with perivascular space widening in both basal ganglia (Figs 5B, -C) and new nodular enhancing lesion in the left parietal lobe (Fig 5D). The malacic cavities, which were seen on the previous 2 serial images in the right temporal periventricular white matter and the right frontal lobe, were unchanged. The patient was treated again with dexamethasone (4 mmg/day for 7 days, 2 mmg/day for 3 days, and 1 mmg/day for 2 days). On the 15-month follow-up MR images, perivascular space widening and subtle enhancement were observed in both basal ganglia (Fig 6A). The left parietal lesion changed to a focal cavity, similar to the right frontal lesions, but subtle enhancement was still noted (Fig 6B). On serial follow-up during a 15-month period, the patient was stable without specific complaint and the level of serum lipid was within normal range.

One-month follow-up MR imaging after treatment. T2-weighted (A) and contrast-enhanced T1-weighted (B) images show focal malacic cavity. Contrast-enhanced T1-weighted images (C and D) show newly developed lesions in right frontal lobe.

Four-month follow-up MR imaging. Focal malacic cavity is seen on T2-weighted (A) and contrast-enhanced T1-weighted (B) images.

One-year follow-up MR imaging. Focal high-signal-intensity spots are seen in left basal ganglia on T1-weighted image (A). Contrast-enhanced T1-weighted images show lesions in both basal ganglia (B) and in left parietal lobe (C).

Fifteen-month follow-up MR imaging. Perivascular space widening with subtle enhancement is noted in both basal ganglia (A) and left parietal lobe (B) on contrast-enhanced T1-weighted images.
Discussion
The development of xanthomas is explained but the escape of serum lipoproteins from the vascular compartment that then enter the surrounding tissue at sites of increased vascular permeability, where macrophages subsequently phagocytize these lipids. Because cholesterol is not degraded, it accumulates within these cells, creating “foamy” macrophages. The extracellular cholesterol crystallizes into clefts and induces an inflammatory reaction with giant cells and resultant fibrosis.1,2 Xanthomas are considered to be specialized granulomas rather than true neoplasms. Intracerebral xanthomas may occur in the perivascular spaces that accompany arteries and arterioles as they penetrate the brain.
Serial MR images in our case revealed the tendency of these xanthomas to occur in the perivascular spaces. Some lesions showed characteristic high signal intensity, which suggests their lipid contents, on T1-weighted images, and variable enhancement was seen on gadolinium-enhanced images. With steroid therapy, masses or nodular enhancing lesions changed into cavitary or malacic areas. In the early stage of the xanthoma formation, “foamy macrophages” may accumulate in the perivascular spaces, so we can detect hyperintense foci in the perivascular spaces of the basal ganglia on unenhanced T1-weighted images. Initial periventricular mass was also iso- to hyperintense on unenhanced T1-weighted images, with corresponding low signal intensity on T2-weighted images, representing their high lipid contents.
One recent article reported a case of intracerebral xanthoma presenting as peripherally enhancing mass in the patient with xanthoma disseminatum, which was a histiocytic disorder occurring in the absence of hyperlipidemia and hypercholesterolemia.5 Because of the rarity of this condition, considerable confusion exists regarding its name and classification in intracranial xanthogranulomatous disease. This lesion, however, was also located in the periventricular deep white matter and the pathogenesis might be the same with our case.
Various therapies, including surgical debulking,2,3 radiation therapy,6 and steroid therapy,5 have been attempted with varying degrees of success. Xanthomas are usually considered as a self-limiting benign disorder,1 so conservative management to control hyperlipidemia is recommended, though the exact relationship between xanthoma formation and the level of serum lipid is not well known. Steroid therapy would be effective for the control of edema and inflammation in mass-forming lesions. In our case, the lesion significantly resolved after initial treatment with administration of steroid and medication for hyperlipidemia. During follow-up, however, multiple lesions recurred and developed without associated hyperlipidemia. Unfortunately, we could not find any references that might explain why the recurrence developed after controlling hyperlipidemia and why intracerebral xanthomas are not often seen in many other patients with hyperlipdemia.
Our report documents intracerebral xanthomas in which multiple nodules show typical distribution along perivascular spaces, with characteristic high signal intensity on T1-weighted images and variable enhancement. The awareness of these MR findings might be helpful for correct diagnosis in the proper clinical setting.
- Received January 17, 2005.
- Accepted after revision March 10, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.