
Abstract
BACKGROUND AND PURPOSE: To prospectively evaluate the signal-to-noise ratio (SNR) improvement in diffusion-weighted imaging (DWI) of the spine with the use of a newly developed non–Carr-Purcell-Meiboom-Gill (non-CPMG) single-shot fast spin-echo (SS-FSE) sequence and its effect on apparent diffusion coefficient (ADC) measurements.
MATERIALS AND METHODS: Twenty-four patients were enrolled after written informed consent. DWI of the spine was obtained with an echo-planar imaging (EPI)-based sequence followed by a non-CPMG SS-FSE technique. SNR and ADC values were measured over a lesion-free vertebral corpus. A quality score was assigned for each set of images to assess the image quality. When a spinal lesion was present, contrast-to-noise ratio (CNR) and ADC were also measured. Student t tests were used for statistical analysis.
RESULTS: Mean SNR values were 5.83 ± 2.2 and 11.68 ± 2.87 for EPI and non-CPMG SS-FSE DWI, respectively. SNR values measured in DWI using parallel imaging were found to be significantly higher (P < .01). Mean ADCs of the spine were 0.53 ± 0.15 and 0.35 ± 0.15 × 10−3 mm2/s for EPI and non-CPMG SS-FSE DWI, respectively. Quality scores were found to be higher for the non-CPMG SS-FSE DWI technique (P < .05). Overall lesion CNR was found to be higher in DWI with non-CPMG SS-FSE.
CONCLUSION: The non-CPMG SS-FSE technique provides a significant improvement to current EPI-based DWI of the spine. A study including a larger number of patients is required to determine the use of this DWI sequence as a supplementary tool to conventional MR imaging for increasing diagnostic confidence in spinal pathologic conditions.
Diffusion-weighted imaging (DWI) is based on the random motion of water protons and is successfully used as an important diagnostic tool in the evaluation of different brain disorders.1-3 With its ability to detect altered water-proton mobility, it may also be useful for the evaluation of spinal disorders. There is a limited amount of research on spinal DWI, and it has been particularly used for the distinction of acute benign osteoporotic from malignant vertebral compression fractures.4,5 There is also current effort to implement DWI in the differential diagnosis of several spinal disorders including infection, metastases and degenerative changes.
Diffusion-weighted images are most commonly collected using acquisition schemes based on single or multishot echo-planar imaging (EPI) methods.6,7 This is due to a relatively good signal-to-noise ratio (SNR) achieved with a low radio-frequency power deposition. On the other hand, EPI-based DWI suffers from artifacts caused by susceptibility changes at tissue boundaries, and from geometric image distortions created by significant eddy currents arising from the large magnetic field gradients used.8 Overall, these EPI-related artifacts have a detrimental effect on image quality and can interfere with diagnostic interpretation.
To overcome these EPI-related artifacts, we chose to use a newly developed non–Carr-Purcell-Meiboom-Gill (non-CPMG) single-shot fast spin-echo (SS-FSE) sequence in DWI of the spine.9 Thus the purpose of this study was to prospectively evaluate the SNR and image quality improvement in the DWI of the spine with the use of this newly developed non-CPMG SS-FSE sequence and its effect on apparent diffusion coefficient (ADC) measurements.
Materials and Methods
Patient Population
This study was approved by our institutional review board. Written informed consent was obtained from all participants. Ten healthy volunteers and 14 patients suspected of having spondylodiskitis, metastases, or compression fractures (6 spondylodiskitis, 6 metastases, 2 benign compression fractures) were enrolled in this study. Age range was between 22 and 73 years, with a mean age of 42 years, in a total of 14 men and 10 women. All patients with metastases had histologically proved extraspinal malignancies (breast cancer [n = 2], lung cancer [n = 4]). In 6 patients with spondylodiskitis, 4 had histologically and/or culture-proved tuberculosis. In 2 patients, brucellosis was diagnosed by the patient's history, and compatible imaging features with positive standard tube agglutination test.
MR Imaging Technique
Patients were examined with a 1.5T superconducting MR system (Signa Excite II; GE Medical Systems, Milwaukee, Wis) using a spinal phase-array coil. Maximum gradient strength and slew rate was 33 mT/m and 120 mT/m/s, respectively. All patients underwent DWI in addition to imaging with a routine lumbar MR protocol. The protocol included sagittal and axial T1-weighted spin-echo (SE) sequences (TR/TE/section thickness/intersection gap/matrix: 400 ms/10 ms/5 mm/1 mm/320 × 224), and a sagittal T2-weighted SE sequence (TR/TE/section thickness/intersection gap/matrix: 3500 ms/100 ms/5 mm/1 mm/320 × 224). Contrast agent was administered to 8 patients, and postcontrast SE T1-weighted images in the axial and sagittal planes were also obtained. Diffusion-weighted images of the spine were obtained in the sagittal plane with an SE-EPI DWI sequence (TR/TE/section thickness/intersection gap/matrix/NEX/b value: 10,000 ms/80 ms/5 mm/1 mm/160 × 160/1/0 and 600 mm2/s), followed by a non-CPMG SS-FSE DWI technique (TR/TE/section thickness/intersection gap/matrix/NEX/b value; 8000 ms/140 ms/5 mm/1 mm/160 × 160/1/0 and 600 mm2/s). The selection of a b value of 600 mm2/s was based on a compromise between signal intensity and adequate diffusion strength. At both b values, the diffusion sensitization was repeated in each orthogonal gradient direction (phase encoding, readout, section selection). All DWI was performed before contrast injection. Imaging time was 48 seconds for SE-EPI-DWI and 40 seconds for non-CPMG SS-FSE DWI.
Image Analysis
All images were analyzed in consensus by 2 experienced radiologists. To assess the visual image quality, an image quality score on a 4-point scale, from 1 (excessive artifact) to 4 (no artifact), was assigned for each dataset. ADC maps were derived automatically on a voxel-by-voxel basis using commercially available software (Advantage Workstation, release 4.1; GE Medical Systems). The ADC was calculated with a linear regression analysis of the function S = S0 exp(−b × ADC), where b is the diffusion factor, S is the signal intensity after application of the diffusion gradient, and S0 is the signal intensity at b = 0 s/mm2.
For quantitative analysis, SNR of a lesion-free vertebral body was measured on both DWI series. SNR was calculated as follows: SNRVertebra = SIVertebra/SDNoise. Vertebral signal intensity (SI) was recorded as the value generated by placing a circular region of interest (ROI) of 1 cm in diameter over the L3 vertebral body on each DWI series. If a lesion was present at L3 vertebra, measurements were completed from the first adjacent normal vertebra. A ROI placed in the most artifact-free air area was taken as the noise, and its standard deviation was used for SNR calculation. ADC values of the normal vertebra were obtained using the same ROIs established for SI measurements.
When a vertebral lesion was present, contrast-to-noise ratio (CNR) and ADC were also measured on both datasets. CNR was calculated as follows: CNR = (SILesion − SIVertebra)/SDNoise. Lesion SI was recorded as the value generated by placing ROIs within the confines of the lesions using T1- and T2-weighted image guidance. ADC values of the lesions were obtained using the same ROIs established for SI measurements.
Statistical Analysis
Statistical analysis was performed with commercially available statistical software (SPSS, 11.0; SPSS, Chicago, Ill). Differences in quantitative analysis results obtained from 2 different DWI datasets were assessed with the paired Student t test. A P value of 0.05 or less was defined as significant.
Results
SNR and ADC values obtained from the normal vertebra with 2 different DWI sequences for a b value of 600 mm2/s, and corresponding image quality scores are shown in Table 1. SNR values associated with non-CPMG SS-FSE technique were found to be significantly higher than those measured with the EPI-based DWI technique (P < .01). ADC measurements obtained with EPI-based DWI were found to be significantly higher than the non-CPMG SS-FSE DWI technique. Image quality scores were found to be higher in non-CPMG SS-FSE DWI technique, compared with the EPI-based DWI sequence. Images of a patient with normal MR imaging findings are shown in Fig 1.

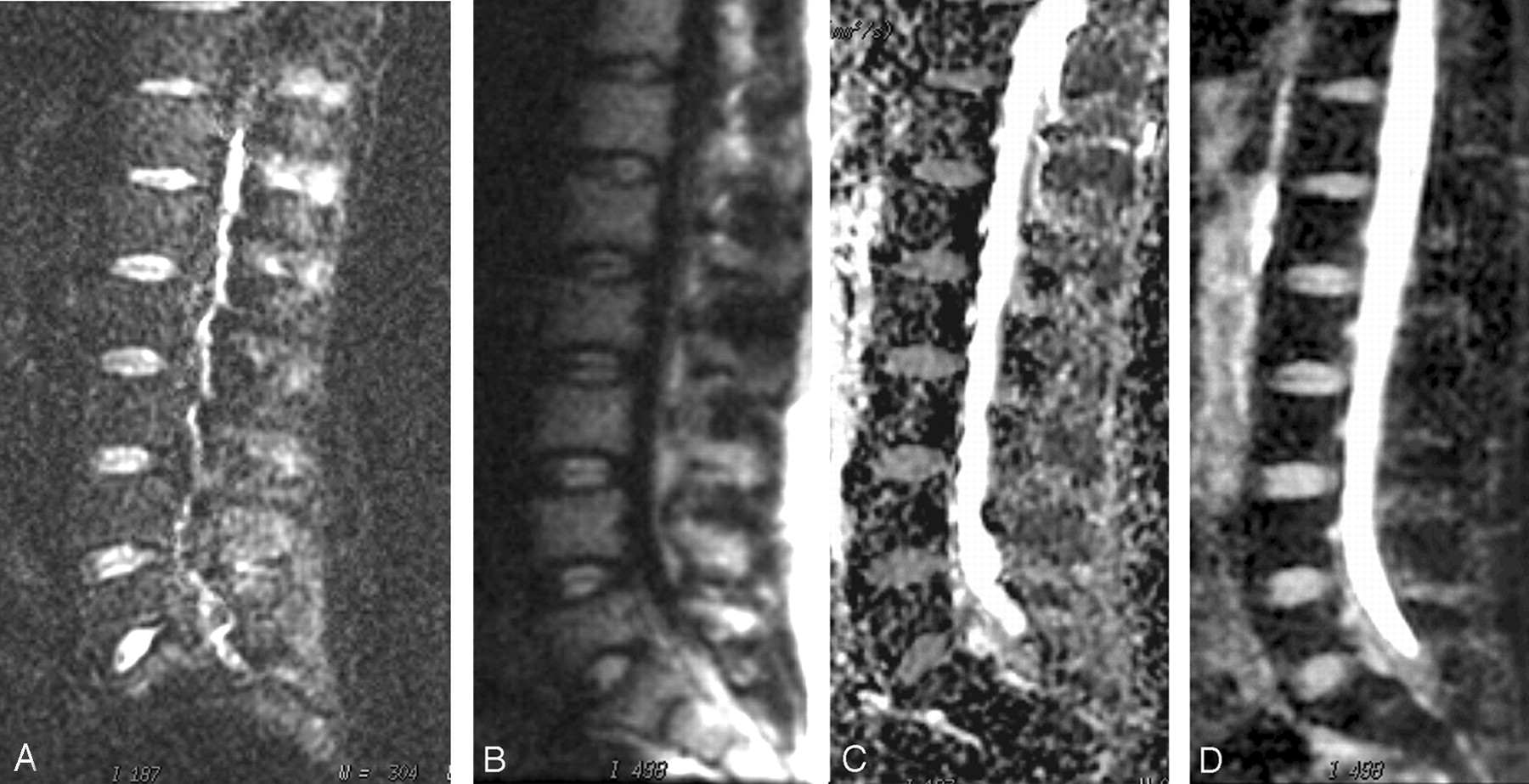
Sagittal diffusion-weighted images in a 25-year-old man with normal spine MR imaging findings obtained at the same level with 2 different techniques: EPI DWI at b = 600 mm2/s (A) and non-CPMG SS-FSE DWI at b = 600 mm2/s (B) and corresponding apparent diffusion coefficient (ADC) maps (C and D, respectively). Increased signal intensity, with better background suppression is noted with the non-CPMG SS-FSE technique. ADC values for the L3 vertebra are (mean ± SD) 0.51 ± 0.17 and 0.37 ± 0.14 × 10−3 mm2/s for EPI and non-CPMG SS-FSE DWI, respectively.
Mean SNR, ADC values and corresponding image quality scores of the normal lumbar vertebra measured by two different DWI sequences
CNR and ADC values for vertebral lesions are shown in Table 2. Overall lesion CNR was found to be higher in DWI using non-CPMG SS-FSE technique. However, statistical analysis based on lesion types was not possible because of the small number of spinal lesions included in this study. Diffusion-weighted images of 3 patients with vertebral lesions are shown in Figs 2, 3, and 4.

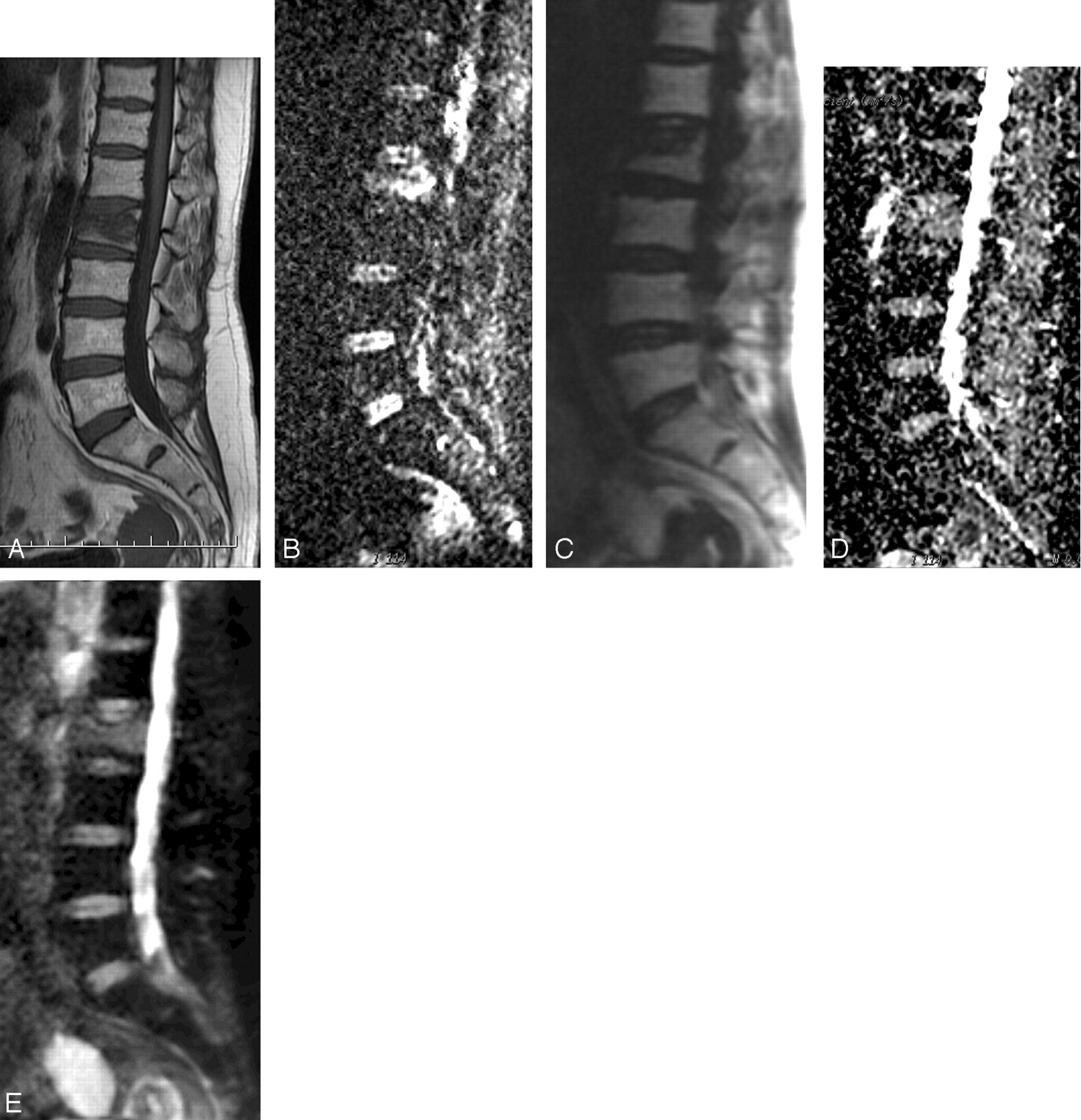
A 46-year-old woman with L2 vertebral compression fracture. Sagittal T1-weighted image (A) and diffusion-weighted images obtained at the same level with 2 different techniques: EPI DWI at b = 600 mm2/s (B), non-CPMG SS-FSE DWI at b = 600 mm2/s (C), and corresponding apparent diffusion coefficient (ADC) maps (D and E, respectively). The compression is more readily appreciated on the non-CPMG SS-FSE images. ADC measured from L3 vertebral body is (mean ± SD × 10−3 mm2/s) 0.54 ± 0.14 and 0.38 ± 0.16 for EPI and non-CPMG SS-FSE DWI, respectively. ADC values measured from L2 vertebra are (mean ± SD) 1.63 ± 0.27 and 1.55 ± 0.24 × 10−3 mm2/s for EPI and non-CPMG SS-FSE DWI, respectively. This reflects the increased diffusion caused by the accompanying bone marrow edema.

A 53-year-old man with Brucella species spondylodiskitis involving the L3–L4 vertebrae. Sagittal postcontrast T1-weighted image (A) and diffusion-weighted images obtained at the same level with 2 different techniques: EPI DWI at b = 600 mm2/s (B), non-CPMG SS-FSE DWI at b = 600 mm2/s (C), and corresponding apparent diffusion coefficient (ADC) maps (D and E, respectively). Postcontrast T1-weighted image demonstrates contrast enhancement in the disk and adjacent vertebral body. Spinal involvement is more readily appreciated on non-CPMG SS-FSE images. ADC measured from L3 vertebral body is (mean ± SD) 1.57 ± 0.14 and 1.31 ± 0.17 × 10−3 mm2/s for EPI and non-CPMG SS-FSE DWI, respectively.

A 56-year-old man with small-cell lung cancer involving T12 and L4 vertebrae. Sagittal postcontrast T1-weighted image (A) and diffusion-weighted images obtained at the same level with 2 different techniques: EPI DWI at b = 600 mm2/s (B), non-CPMG SS-FSE DWI at b = 600 mm2/s (C), and corresponding apparent diffusion coefficient (ADC) maps (D and E, respectively). Postcontrast T1-weighted image demonstrates mild contrast enhancement at T12 and L4 vertebral body. High signal intensities over T12 and L4 vertebrae are observed on both diffusion images. ADC measured from T12 vertebral body is (mean ± SD) 0.74 ± 0.14 and 0.70 ± 0.17 × 10−3 mm2/s for EPI and non-CPMG SS-FSE DWI, respectively.
Mean CNR and ADC values measured by two different DWI sequences in spinal lesions
Discussion
DWI measures the mobility of tissue water on a microscopic level and has gained wide acceptance in the management of various central nervous system disorders. Several potential fields of application were also reported in the medical literature, including musculoskeletal system, bone marrow, and abdominal organs.5,10-12 Because of the relatively good SNR achieved, EPI-based sequences are the most widely used DWI techniques. Unfortunately, these EPI-based diffusion-weighted images suffers from susceptibility artifacts and image distortion caused by eddy currents resulting from the large magnetic field gradients.
The need for artifact-free DWI has prompted research into other methods, such as a single-shot DWI based on the rapid acquisition with relaxation enhancement (RARE).13 A RARE acquisition scheme use a series of radio frequency (RF) refocusing pulses rather than gradient reversals to produce echo trains and therefore has a much lower sensitivity to eddy currents, chemical shift artifacts, and susceptibility gradients than the EPI technique.8 However, the RARE method must obey the CPMG14 phase condition and, when it is used with diffusion sensitization, cannot generate artifact-free images because of uncontrolled phase modulations. The strong sensitivity of the sequence to the CPMG condition can be suppressed but at the price of a reduction of the SNR by a factor of 2.15 Le Roux9 has addressed this signal intensity loss in DWI by using a non-CPMG SS-FSE technique that uses quadratic phase modulation of the RF refocusing pulses to generate a sustained train of stable echoes. This results in a DWI technique less sensitive to eddy currents and magnetic field inhomogeneities without any apparent signal intensity loss.
In the current study, the non-CPMG SS-FSE technique resulted in higher quality diffusion images with a lesser degree of distortion and susceptibility related artifacts as reflected in the visual image quality assessment scores. Our preliminary results suggest that the non-CPMG SS-FSE sequence can be used to improve SNR of spine DWI by decreasing eddy currents and susceptibility related artifacts without any time penalty. ADC values of the normal vertebral bone marrow measured with the 2 different techniques were within the limits defined by previous studies.11,16-18 On the other hand, the difference in the ADC measurements found between the 2 different DWI techniques in this study is not surprising. In fact, the accuracy of ADC values depends on many factors, such as the SNR, spatial resolution, and the number and amplitude of the b values used in the data acquisition.18 In this setting, with the other parameters, including the b values, being the same, the increased SNR in the non-CPMG SS-FSE technique is the primary source of difference for the ADC measurement between the 2 DWI methods. It might also be hypothesized that, because of decreased susceptibility-related artifacts, quantitative measurements with this new technique better reflect diffusion properties of the spine.
The spine is commonly involved in various pathologic processes. Sometimes it is hard to make a confident differential diagnosis by conventional MR imaging for definitive treatment. In these circumstances, DWI may be a helpful technique to outline the undergoing process. Any pathologic process, whether neoplastic, inflammatory, or degenerative, may disturb normal tissue architecture and cause ultimate shifting of water molecules between tissue compartments secondary to disruption of cellular structure and membranous permeability or both.19
Although there are still some conflicts, differentiation of benign vertebral compression from its malignant counterpart is one of the most promising applications of spine DWI. Increased diffusion of interstitial water is a common phenomenon and may be observed in acute posttraumatic edema of the bone resulting in low signal intensity on DWI.20 In contrast, densely packed tumor cells restrict the diffusion, resulting in lower phase shift with high signal intensity on DWI.4 However, these SI changes are not solely related to diffusion alterations, but they are also greatly influenced by the T2 shine-through. Therefore, qualitative assessment of DWI alone is not adequate and ADC measurements are crucial in the demonstration of diffusion alterations. Unfortunately, there were no examples of vertebral collapse as a result of malignant infiltration in the limited number of patients presented in this article. However, ADC values of 2 patients with benign vertebral compression were found to be higher than the normal vertebral bone marrow. This reflects the increased diffusion caused by the accompanying bone marrow edema and is in good concordance with the values reported in the literature.17
A second promising application of spine DWI can be in the differential diagnosis of different spinal disorders, including infection, metastases, and degenerative changes. MR imaging has evolved as the diagnostic method of choice in these groups of patients because of its excellent tissue contrast.21,22 Although sensitive, the specificity of MR imaging is limited because of similar signal intensity changes in both neoplasia and benign conditions such as inflammation, degeneration, post-traumatic edema, or infectious process.20,23 Initial studies used qualitative assessment of DWI alone without ADC measurements but resulted in conflicting imaging characteristics because of the T2 shinethrough on diffusion images.21,23,24 To eliminate the T2 shinethrough effect from the diffusion images, a few studies used ADC mapping and measurements but failed to demonstrate any significant difference in terms of ADC between various pathologic bone marrow conditions.4,25 However, these quantitative studies used EPI-based DWI techniques, which are more sensitive to eddy currents and susceptibility artifacts. These constraints might have contributed to the failure to demonstrate ADC differences between various spinal pathologies. Based on initial data obtained over a limited number of patients, the above presented non-CPMG SS-FSE DWI technique can be promising in the quantitative evaluation of various spinal pathologies.
A main limitation for our study is that only a small number of patients with spinal lesions were studied. Measured lesion CNR was found to be higher on non-CPMG SS-FSE DWI, reflecting improved lesion conspicuity. Compared with infectious process and benign compression fractures, metastases had lower ADC values. This reflects an emphasized water restriction caused by the tumor packing. Compared with benign compression fractures, the slight ADC decrease observed in infectious process is more apparent on non-CPMG SS-FSE images. This difference can be explained by the increased cellular content accompanying bone marrow edema in infection. However, the number of vertebral lesions included in this study is too small to statistically analyze and to set a threshold ADC value to make a differential diagnosis. Therefore, further studies with larger numbers of patients are needed in the future.
In conclusion, the non-CPMG SS-FSE technique, with its reduced susceptibility artifacts and increased SNR, provides a significant improvement to current EPI-based DWI of the spine and may be useful as a supplementary tool to conventional MR imaging for increasing diagnostic confidence in spinal pathologies.
Footnotes
Poster previously presented at: Annual Meeting of the American Society of Neuroradiology, April 29–May 5, 2006; San Diego, Calif.
References
- Received March 14, 2006.
- Accepted after revision May 8, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.