
Abstract
Summary: Proper assessment of endovascular patency after carotid stent (CS) placement with carotid color-coded duplex sonography (CCCD) can be difficult. We investigated the usefulness of contrast-enhanced (CE) CCCD for post-CS follow-up. CCCD images could not depict the entire bloodstream in overlapped stents and in highly positioned stents. CE-CCCD images, however, did provide anatomic information almost equivalent to that of intra-arterial angiography. CE-CCCD is useful in screening for post-CS restenosis.
Carotid stent (CS) placement is a new procedure that is gaining increasing popularity for the treatment of carotid stenosis. It is now being investigated as an alternative to carotid endarterectomy (1–5). The long-term results of CS placement, however, have been poorly documented, and this lack reinforces the necessity of repeat follow-up assessments after CS placement (1, 3–5).
Doppler sonography is a noninvasive and easily repeatable investigation. Carotid Doppler scanning for the evaluation of the carotid circulation, however, has some limitations. A patient with a short neck or a high carotid bifurcation often cannot be fully imaged by means of conventional Doppler imaging (6, 7). In addition, the blood flow in the residual lumen in patients with high-grade carotid stenosis cannot be detected because of sonographic absorption by the atheroma. Furthermore, in patients who undergo CS placement for the treatment of carotid artery stenosis, endovascular prostheses make sonographic penetration difficult (8).
A relatively new development that can overcome these limitations is the application of contrast enhancement in combination with carotid color-coded duplex (CCCD) sonography (7, 9, 10). Levovist (Schering, Berlin, Germany) is the most popular echocontrast agent used in neurosonography. When mixed with water and administered intravenously, it results in air-filled microbubbles (with a mean diameter of 3 ìm) covered by a thin layer of palmitic acid. Echocontrast agents that produce transpulmonary, stable microbubbles increase the echogenicity of arterial blood flow and improve the signal-to-noise ratio of Doppler signals.
The aim of the present study was to evaluate the benefit of contrast-enhanced (CE) CCCD for the follow-up assessment after CS placement in patients with carotid artery stenosis.
Technique
Fifteen consecutive patients (12 men and three women) (Table) who underwent CS placement in our institute were examined with carotid sonography. The mean age of the patients was 69.7 years, with a range of 55 to 79 years. A total of 17 CS procedures were performed in 15 carotid arteries by using either self-expanding stents (Smart stent; Johnson and Johnson, Warren, NJ) for seven procedures or balloon-expandable stents (Palmaz stent, Johnson and Johnson; Wiktor stent, Medtronic, Minneapolis, MN) for 10 procedures. Overlapped stents were placed in two patients to achieve an adequately smooth hemodynamic result.
Summary of CS procedures, follow-up findings, and depiction of the stented lumen at CCCD and CE-CCCD sonography
A sonography system with a 5–12-MHz linear probe (ATL HDI 5000; Hitachi, Tokyo, Japan) was used to perform imaging of the carotid arteries. Patients sequentially underwent CCCD and CE-CCCD examinations performed by experienced technicians. In each sonographic procedure, the gain setting was set high enough to detect as much flow in the stent as possible, and it was set low enough to avoid color bleeding into surrounding tissue. Both CCCD and CE-CCCD investigations were continuously recorded on VHS videotape for offline analysis. Images of particular interest were also printed.
One 2.5-g vial of the echo-enhancer Levovist (7 mL suspension; Schering) was intravenously administered in a concentration of 300 mg/mL via an 18-gauge catheter placed in the antecubital fossa. In the initial five patients, two ways of administering the echocontrast were tried separately, and the resulting images were compared. These patients were given a manual bolus injection of the echo-enhancer (at a rate of approximately 1 mL/s) before the first set of images were acquired, and they were then given a continuous infusion by means of a pump injector at a rate of 1 mL/min for the second set of images. For the next 10 patients, CE-CCCD images were obtained only by using the infusion method.
All patients except one (patient 6) underwent intra-arterial digital subtraction angiography of the carotid arteries within a short time of the sonographic investigations. Blood flow within the stents, as depicted by using CCCD and CE-CCCD were compared with that assessed by using DSA (Table). Three independent observers, each blinded to the other two readers’ findings, analyzed the results of CCCD (K.Y.), CE-CCCD (K.N.), and DSA (K.K.). The mean interval between DSA and sonography was 26.8 hours, with a range of 3 to 72 hours.
This study was approved by the hospital ethics committee, and informed consent was obtained from all patients.
Results
None of the contrast agents caused any adverse effects. In the initial five patients who were examined by means of both a continuous infusion and a bolus injection of the echo-enhancer, CE-CCCD images produced with the continuous infusions provided stable visualization of the blood flow in the stent. In all cases, the contrast enhancement lasted until the end of the infusion. On the other hand, three of five CE-CCCD images produced with the bolus injection caused contrast agent-related artifacts (eg, color blooming), and they provided only a short echo-enhancement time (average, 1.2 minutes). Therefore, the native CCCD images were compared with only the CE-CCCD images produced with the infusion of contrast medium when we analyzed the diagnostic benefit of the CE-CCCD examinations.
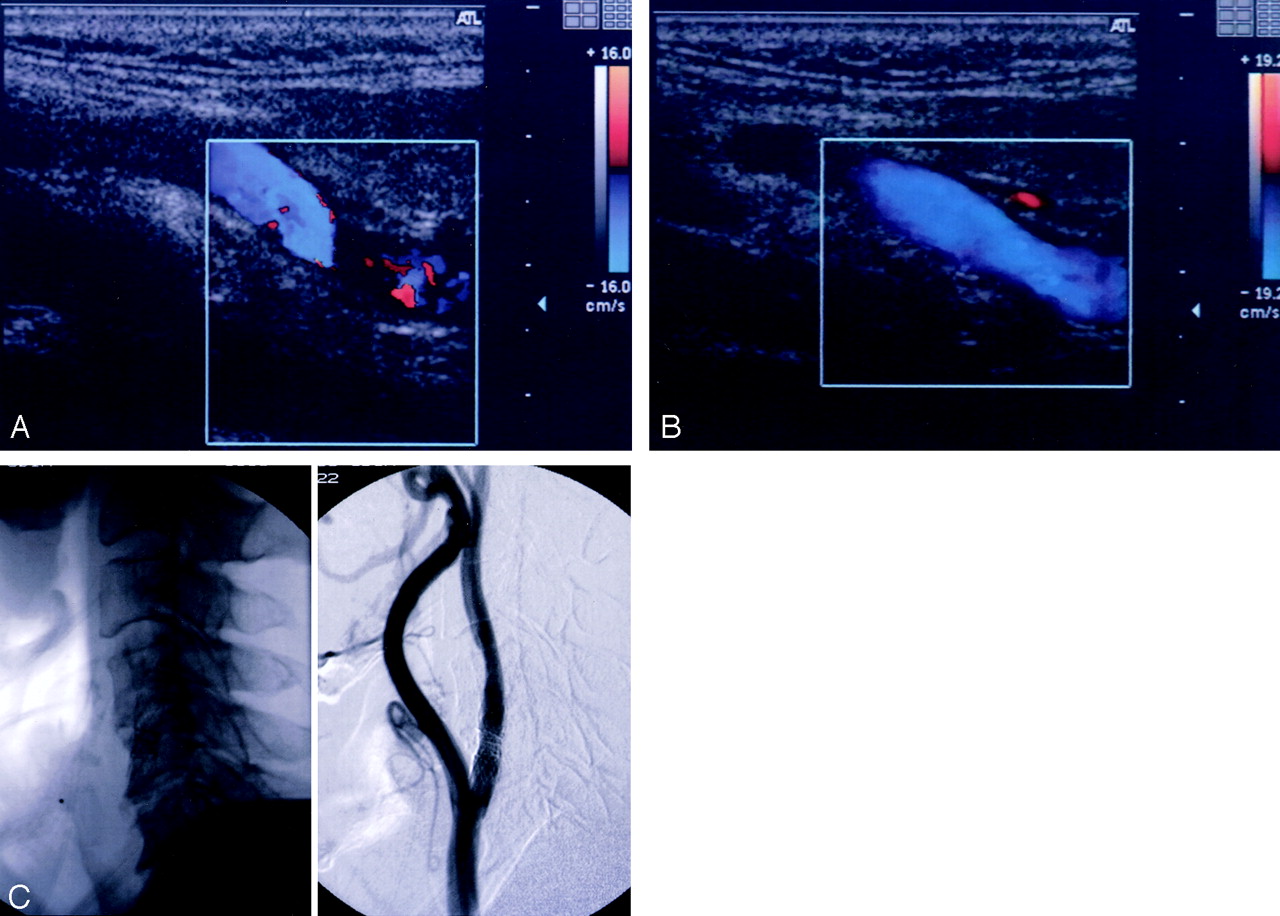
In the two patients who underwent overlapped stent placement, none of the original CCCD images completely showed flow in the stents. After the administration of the contrast agent, continuous visualization of the color-coded bloodstream, even in the overlapping part of the stents, was possible. These CE-CCCD images provided anatomic information almost equivalent to that possible with angiography (Fig 1).

Benefit of CE-CCCD sonography in a patient with overlapped stents (patient 14).
A, Nonenhanced CCCD image did not allow visualization of blood flow in the overlapped stents.
B, CE-CCCD sonogram provides anatomic information almost equivalent to that on the DSA image.
C, Corresponding lateral radiograph (left) and DSA (right) images.
In five of the 13 patients who underwent CS placement with a single stent, the CCCD image and the CE-CCCD image differed significantly in the visualization of the entire length of the flow in the stent. These five patients had high carotid lesions (Fig 2). In the nine patients whose stent was located below the level of the second vertebra, nonenhanced CCCD images allowed full confirmation of stent patency (Table). With CE-CCCD sonography, improvement in the visualization of blood flow in a stent did not depend on the stent material (Table). In patient 4, an asymptomatic intimal hyperplastic narrowing of approximately 50% of the lumen was confirmed by means of DSA after successful CS placement. However, this intrastenotic residual lumen could not be visualized on the CE-CCCD images, although a more color-coded stream was shown proximal and distal to the stenotic portion.

Benefit of CE-CCCD sonography in a patient with a high cervical lesion (patient 5).
A, Nonenhanced CCCD image allowed visualization of only the proximal half of the stented lumen.
B, After the application of the contrast agent, flow in the distally positioned stent could fully be detected by means of CE-CCCD imaging.
C, Corresponding lateral X-p (left) and DSA (right) images.
Discussion
Angiography has been regarded as the criterion standard for immediate and postinterventional follow-up. However, most clinicians rarely perform repeat angiography because of its several drawbacks. First, angiography can be potentially harmful. Complications include death, contrast material–induced shock, stroke, arterial injury, and renal failure (11). Second, angiography is a costly technique. In Japan, the cost of angiography is roughly 12 times that of CCCD imaging and four times that of CE-CCCD imaging. Sonography, on the other hand, has several advantages in the assessment of vascular lesions. It is less invasive, highly accurate, easily repeatable, and cost-effective. In addition, Doppler sonography can provide not only anatomic but also real-time functional information. However, nonenhanced CCCD investigations are occasionally inadequate in the evaluation of carotid artery disease, as approximately 10% of patients cannot be successfully imaged (6) because of anatomic factors such as high carotid bifurcations and short necks. In addition, after CS placement, endovascular prostheses can often make sonographic penetration difficult (9).
In this study, about half of the stented carotid lumens without stenosis were not completely visualized by means of the nonenhanced CCCD scans. In these cases, CE-CCCD investigations could fully depict blood flow within the stents. Patients in whom precontrast images afforded poor visualization of the stented carotid lumens were those who had overlapped stents or who had high cervical lesions. In the former, overlap of the stents may have prevented insonation. In the latter, the long distance between the probe and the artery, in addition to an unfavorable insonation angle, may have contributed to the incomplete assessment. Echocontrast agents that are capable of improving the signal-to-noise ratio play an important role in overcoming these limitations.
In our initial five cases, we compared two methods of contrast agent administration for CE-CCCD imaging. We found that continuous infusion is diagnostically superior to bolus injection because of its uniform and prolonged enhancement without saturation artifact.
Contrast agent–related adverse effects reported in the literature (12) are minor and transient, and they are not associated with observable adverse effects, irrespective of the mode of administration. Thus, CE-CCCD investigation is almost as safe as sonographic scanning without the use of a contrast medium.
Although based on a limited number of patients, our results suggest that the visualization of the flow in a stent with luminal narrowing, as indicated by the color-flow signal intensity in the intrastenotic residual lumen, cannot be detected on CE-CCCD images if the stenosis is greater than 50%. Thus, in the evaluation of a stented lumen with stenosis, CE-CCCD imaging may pose a risk of underestimating its patency. Therefore, in cases with stenosis, DSA is superior to Doppler sonography in its diagnostic accuracy. Because we had only one case in which a stented lumen was narrowed by intimal hyperplasia, the flow parameters (eg, peak systolic velocity and diastolic velocity) between stented lumens with and those without recurrent stenosis cannot be compared. Further studies involving a larger number of patients with severe stenosis are required to elucidate the relationship between the CE-CCCD findings in stented lumens and the degree of stenosis. According to our preliminary results, CCCD images could not completely depict flow in the stents in approximately one-half of the patients without restenosis after CS placement. CE-CCCD sonography, however, improved blood flow images in the stents and provided anatomic information almost equivalent to that obtained with angiography. Therefore, DSA may be an appropriate follow-up investigation after CS placement, but only in cases in which flow in the stented lumen cannot be confirmed with CE-CCCD sonography.
References
- Received June 10, 2002.
- Accepted after revision November 26, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.