
Abstract
BACKGROUND AND PURPOSE: Basal cell adenomas (BCAs) are rare tumors of the parotid gland. Only a few case reports describing MR imaging features of BCA have been published. The aim of this study was to describe and characterize the MR findings of BCAs of the parotid gland.
MATERIALS AND METHODS: We retrospectively reviewed MR images of BCA with pathologic correlation in 8 cases (2 men and 6 women; age range, 52–82 years) collected between January 1992 and August 2004 from our pathologic data base. All MR images were retrospectively evaluated with respect to the marginal morphology, signal intensity (SI), and enhancement behavior by 2 experienced radiologists.
RESULTS: On pathologic examination, 5 tumors were solid type, 2 were trabecular type, and 1 was membranous type. All of the tumors were well circumscribed with smooth contours. Cystic changes were seen in 4 cases. On T1-weighted images (T1WI), 7 tumors showed homogeneously low SI equal to muscle and one showed heterogeneously low SI. On T2-weighted images (T2WI), all of them showed slightly lower SI than that of surrounding parotid tissue. On gadolinium-enhanced T1WI, 6 tumors demonstrated moderate enhancement and one demonstrated strong enhancement (membranous type). Dynamic studies were performed in 4 cases. All showed rapid and prolonged enhancement.
CONCLUSION: MR imaging findings of BCA were well-defined and smooth marginal morphologies, relatively low SI on both T11W and T2WI, and rapid and prolonged enhancement on dynamic study. Although BCAs are rare, they should be suspected when a tumor shows all of the characteristics noted here.
Basal cell adenomas (BCAs), as defined by the World Health Organization, are a distinctive benign neoplasm composed of basaloid cells organized with a prominent basal cell layer and distinct basement membrane-like material.1 BCAs account for 1%–2% of all salivary gland epithelial tumors, and >80% arise in the major salivary glands, mostly the parotid gland. BCAs are pathologically classified into 4 subtypes according to their cellular growth pattern: solid, tubular, trabecular, and membranous.2
Because of their low prevalence, there are few reports regarding imaging findings of BCAs in the parotid gland. This study aimed to describe and characterize MR findings of BCAs of the parotid gland and correlate these with pathologic findings.
Materials and Methods
Patients
We retrospectively reviewed MR images of BCAs with pathologic correlation in 8 cases (2 men and 6 women; age range, 52–82 years; mean age, 66 years) collected between January 1992 and August 2004 from our pathologic data base.
MR Imaging Technique
MR images were obtained with a 1.5-T scanner (Signa; GE Medical Systems, Milwaukee, Wis or Magnetom; Siemens Medical System, Erlangen, Germany) with quadrature head coils. Transverse images were obtained by using the fast spin-echo (FSE) technique. T1-weighted (T1WI; 400–660/9–20 [repetition time milliseconds/echo time milliseconds]) and T2-weighted images (T2WI; 2000–4000/100–110) were obtained for all patients. After intravenous injection of a solution of gadopentetate dimeglumine (0.2 mL/kg), transverse and coronal T1WI (400–600/10–20) were obtained for 7 patients (only one patient by using fat suppression to postgadolinium [Gd]-T1WI). Dynamic study (by using fast multiplanar spoiled gradient echo [170/4.2]; scan timing was precontrast, 20 seconds, 60 seconds, 120 seconds, and 180 seconds) was performed in 4. Section thickness was 6 mm with a gap of 1 mm, and the acquisition matrix was 256 × 256 or 256 × 192.
Image and Pathologic Analysis
All MR images were retrospectively evaluated with respect to size, location, the marginal morphology, signal intensity (SI), and enhancement behavior by 2 experienced radiologists. Consensus was always obtained in cases of discrepancy between both readers. An experienced radiologist and a pathologist correlated the MR images and pathologic specimens.
Results
MR Imaging Findings
Size, Location, and Marginal Morphology.
The average maximal cross-sectional diameter was 2.8 cm (range, 1.0–5.8 cm). Seven tumors were located in the superficial lobe of the parotid gland and one was located in the deep lobe of the parotid gland (Table). All tumors had well-defined margins with smooth contours. On T1WI and T2WI, a capsule-like low-SI rim was detected in only one tumor.
Summary of results
SI and Enhancement Behavior.
Large cystic changes were seen in 4 tumors. On T1WI, 7 showed homogeneously low SI equal to muscle and one showed heterogeneously low SI. On T2WI, all of the solid parts of the tumors showed slightly lower SI than that of the surrounding parotid tissue. On Gd-enhanced T1WI, the solid part of 6 demonstrated moderate enhancement and one demonstrated marked enhancement (membranous type). On dynamic study, 4 showed rapid and prolonged enhancement.
Pathologic Findings
On pathologic examination, 5 tumors were classified as solid type, 2 as trabecular, and one as membranous. All tumors were well circumscribed and had a thin fibrous capsule. Cystic changes were seen in 4 tumors, and 4 solid and one membranous type had numerous endothelial-lined vascular channels.
Discussion
A BCA is a distinctive benign neoplasm composed of basaloid cells organized with a prominent basal cell layer and distinct basement membrane-like material and lacking the fibromyxoid stromal component of pleomorphic adenoma. BCAs account for 1%–2% of all salivary gland epithelial tumors1 and >80% arise in the major salivary glands, mostly the parotid gland.3 On pathologic examination, various degrees of cystic changes were seen in 65% of cases of BCAs.4 They have characteristic, numerous, endothelial-lined vascular channels, in which small capillaries and venules are prominent, which can explain why BCAs are well-enhanced.
BCAs have 4 pathologic subtypes: solid, trabecular, tubular, and membranous type.2 Solid, the most common subtype, is characterized by aggregates of epithelial tumor cells arranged as large sheets or nodules separated by various amounts of stromal tissue.2 The trabecular type is evinced by an interlacing network of narrow bands of basaloid cells, which are punctured by a few or many small cysts or ductal lumens in some tumors. Some investigators have considered trabecular and tubular types as one tubulotrabecular type.4 Duct cell differentiation is most prominent in the tubular type, which is the least common type of BCA. The most characteristic feature of the membranous type is the production of a conspicuous amount of basal lamina that is recognized as an eosinophilic, Periodic acid-Schiff (PAS)-positive hyaline material, which forms thick bands at the periphery of the basaloid cell islands.2 In contrast to the other types of BCAs, the membranous type has a high recurrence rate of 25%–37%, probably because of its tendency to be multilobulated and unencapsulated.5 Therefore, the membranous type of BCA should be classified separately from other BCAs. In our study, only one case was membranous type, which showed stronger enhancement than the other types of the tumors. Size, morphology, and SI could not distinguish this type and the other subtypes. This enhancement behavior might be one characteristic MR finding for the membranous type (Fig 1).

A 82-year-old man with basal cell adenoma (BCA) (membranous type, marked enhancement)
A, A T1-weighted image (T1WI) shows a homogeneously low-SI mass with a well-defined, smooth margin in the superficial lobe of the left parotid gland.
B, On T2WI, the tumor shows slightly lower SI than the normal parotid gland.
C, On Gd-enhanced fat-suppressed T1WI, the tumor shows homogeneous and strong enhancement.
D, On dynamic study, the tumor shows a rapid and prolonged enhancement pattern.
E, Microscopic examination (hematoxylin-eosin stain [H&E]) shows conspicuous hyaline matrix surrounding epithelial cells. Relatively large vessels are seen in the tumor (arrows).
Few imaging findings of BCA of the parotid gland have been reported.6–9 In our cases, the morphology of BCAs was a well-defined margin and rounded contour, as with cases in previous reports. High-grade malignant tumors can easily be differentiated from BCAs by the infiltrative margins of malignant tumors. The differential diagnosis of BCA includes pleomorphic adenoma, Warthin tumor, and low-grade malignant tumors. Most pleomorphic adenomas have an area containing abundant fibromyxoid stroma, which shows bright SI on T2WI as well as marked enhancement on postcontrast images. These areas show delayed enhancement on dynamic study. In addition, pleomorphic adenomas show lobulated contours and typically have a thick capsule.9–11 These characteristic MR findings of pleomorphic adenoma are helpful for differentiation between pleomorphic adenomas and BCAs. Some pleomorphic adenomas consist of mostly high cellular component but do not have this characteristic bright SI on T2WI. Relatively large cystic changes were seen in half of the cases in our study (Fig 2); these changes are more frequently in BCA than in pleomorphic adenomas.

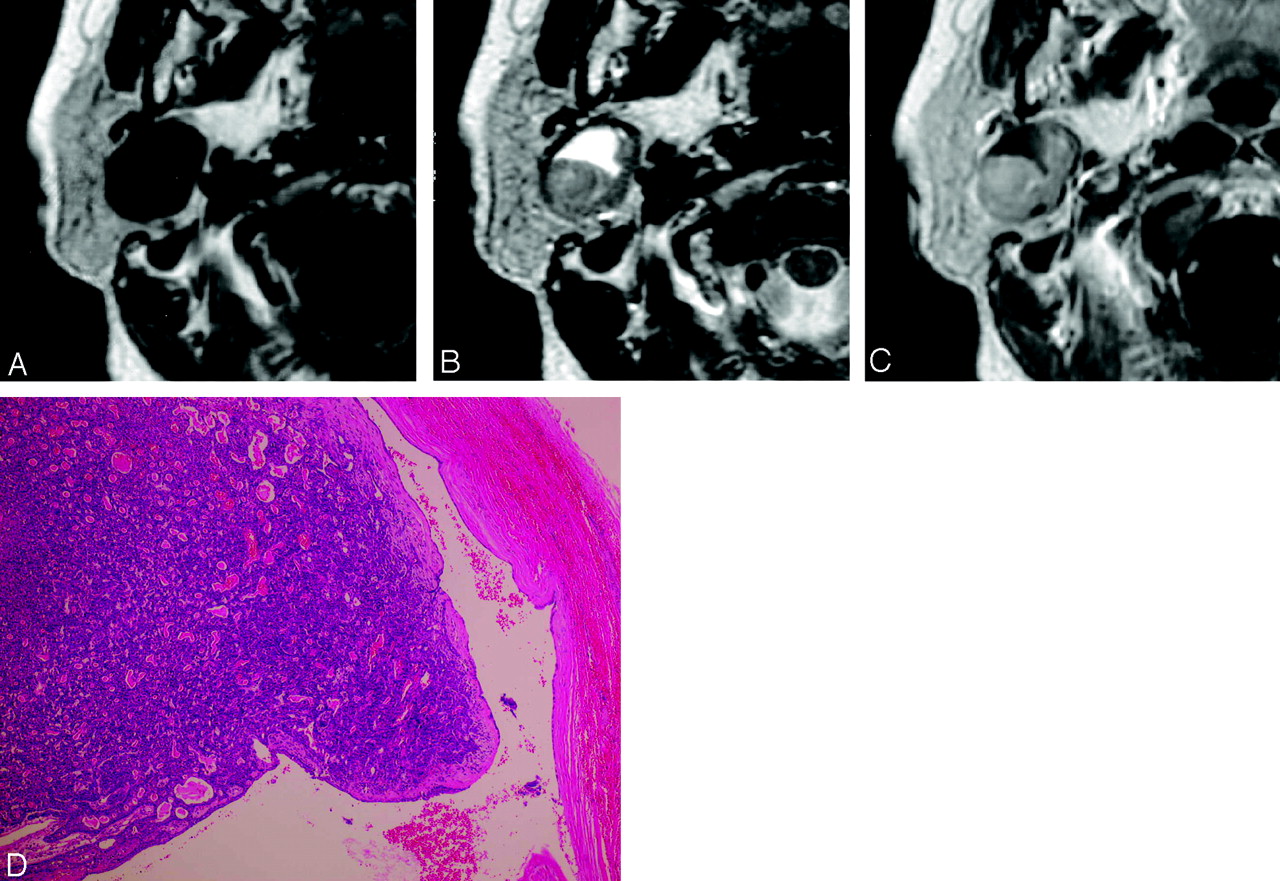
A 68-year-old woman with basal cell adenoma (BCA) (solid type, large cystic change)
A, A T1-weighted image (T1WI) shows a homogeneously low-SI mass with well-defined and smooth margin in the deep lobe of the right parotid gland.
B, On T2WI, the tumor shows slightly lower SI than the normal parotid gland with very high SI (cystic change) at the anterior half of the tumor.
C, On Gd-enhanced T1WI, the tumor shows homogeneous moderate enhancement of the solid component. On T2WI, a very-high-SI area is not enhanced.
D, Microscopic examination (hematoxylin-eosin stain [H&E]) shows a solid pattern with many microcystic changes around a large cystic change. Dilated vascular channels are prominent.
Warthin tumors typically show round or oval contours, low SI on T1WI, and slightly lower SI than that of surrounding parotid tissue on T2WI. These features are similar to BCAs; however, Warthin tumors show early enhancement and early washout pattern on dynamic study,9,12,13 whereas BCAs showed rapid and prolonged enhancement patterns on dynamic study in our cases (Fig 3). In addition, parotid scintigraphy by using technetium Tc99m-pertechnetate is useful for diagnosis of a Warthin tumor.14 Warthin tumors can also show as an almost cystic lesion, the same as BCAs.9

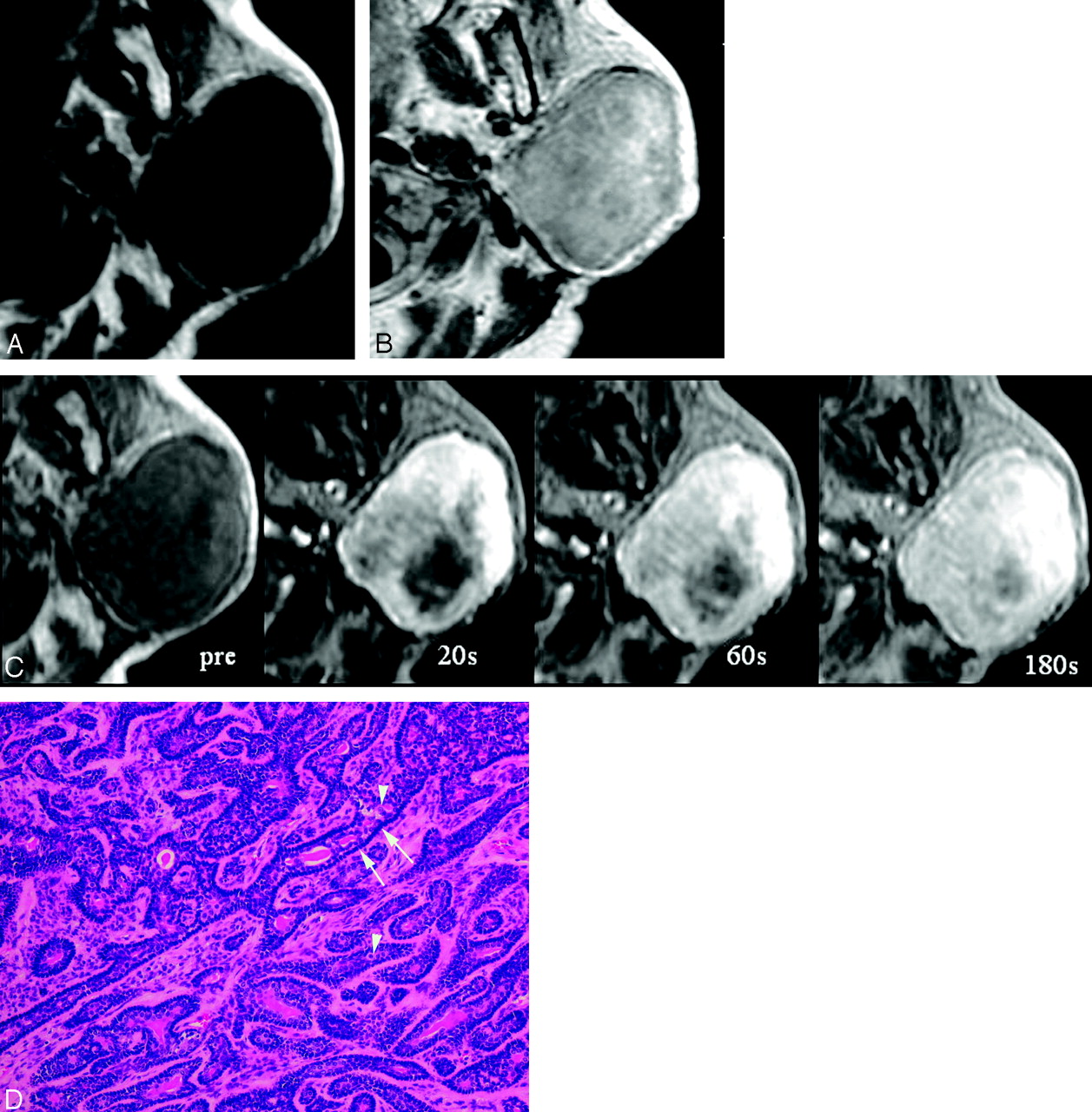
A 69-year-old woman with basal cell adenoma (BCA) (trabecular type)
A, A T1-weighted image (T1WI) shows a homogeneously low-SI mass with a well-defined, smooth margin in the left parotid gland.
B, On Gd-enhanced T1WI, the tumor shows inhomogeneous moderate enhancement.
C, On dynamic study, the tumor shows rapid enhancement at the periphery of the tumor and is gradually enhanced from the periphery to central part of the tumor.
D, Microscopic examination (hematoxylin-eosin stain [H&E]) shows a trabecular pattern of a BCA. The tumor is composed of small uniform basaloid cells (arrowheads) arranged in solid or trabecular pattern. The stroma is loose, scantily collagenous tissue. There is characteristic palisading (arrows) in the peripheral portion of the tumor cell nests.
Low-grade malignant tumors usually demonstrate similar MR findings to benign tumors. Imaging findings are usually nonspecific and indistinguishable from those of benign parotid tumors. Low-grade adenoid cystic tumors, however, show relatively high SI on T2WI,15 which should be useful for differentiating BCAs from low-grade adenoid cystic carcinomas.
Conclusion
MR imaging findings of BCAs were well-defined and smooth marginal morphologies, dissimilar to the lobulated contour seen in pleomorphic adenomas, relatively low SI on both T1WI and T2WI, and rapid and prolonged enhancement on dynamic study. Although BCAs are a rarity, they should be suspected when a tumor shows all of the characteristics noted here.
References
- Received March 27, 2005.
- Accepted after revision August 10, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.