
Abstract
SUMMARY: A 69-year-old woman developed acute pain in the left trigeminal and glossopharyngeal nerve distributions. MR imaging demonstrated a left lateral medullary infarction (LMI) involving the left spinotrigeminal nucleus and tract, nucleus ambiguus, and solitary nucleus. Most patients presenting with trigeminal neuralgia will have disease involving the trigeminal nerve or ganglion or the primary sensory nucleus in the pons. We discuss the unusual finding of LMI associated with concurrent trigeminal and glossopharyngeal neuralgia.
Trigeminal neuralgia (TN) is described as an abrupt unilateral shocklike facial pain lasting seconds to minutes. Episodes can recur multiple times per day and are typically initiated by specific stimuli, such as light touch, smiling, tooth brushing, and chewing.1 Eighty percent to 90% of cases are related to vascular compression of the trigeminal nerve root.1,2 Other reported causes include multiple sclerosis, aneurysm, or tumor.1,3 MR imaging evaluation is performed in patients with TN associated with other cranial nerve signs, such as in this patient with associated glossopharyngeal neuralgia (GPN), to identify a structural lesion.
We discuss an unusual case of concomitant TN and GPN as a sequela of lateral medullary infarction (LMI). We also describe the most common MR imaging findings associated with TN and GPN in context with this unique case, emphasizing the need to include careful examination of the medulla.
Case Report
A 69-year-old woman developed sudden left facial pain while shopping. The pain began in her left temple extending into the left ear, cheek, and jaw. The pain was intense, burning, and sharp and was exacerbated by light touch. Results of emergency CT and subsequent MR imaging (1 week later) performed at an outside institution were reported to be normal. The patient was treated empirically with valacyclovir hydrochloride for suspected herpes zoster without relief. Subsequent trials of gabapentin 600 mg 3 times daily and oxycarbazepine 300 mg twice daily also provided no relief, and the patient was referred to our institution for consideration for trigeminal nerve ablation. At that time, the patient had continued attacks of pain lasting minutes to hours involving the left cheek, ear, and pharyngeal wall. This pain worsened with chewing on the left side and swallowing. The patient had undergone a 15-pound weight loss since the onset of symptoms. There was no ptosis. Pupils were symmetric. She had diplopia looking to the right. There was no skin rash.
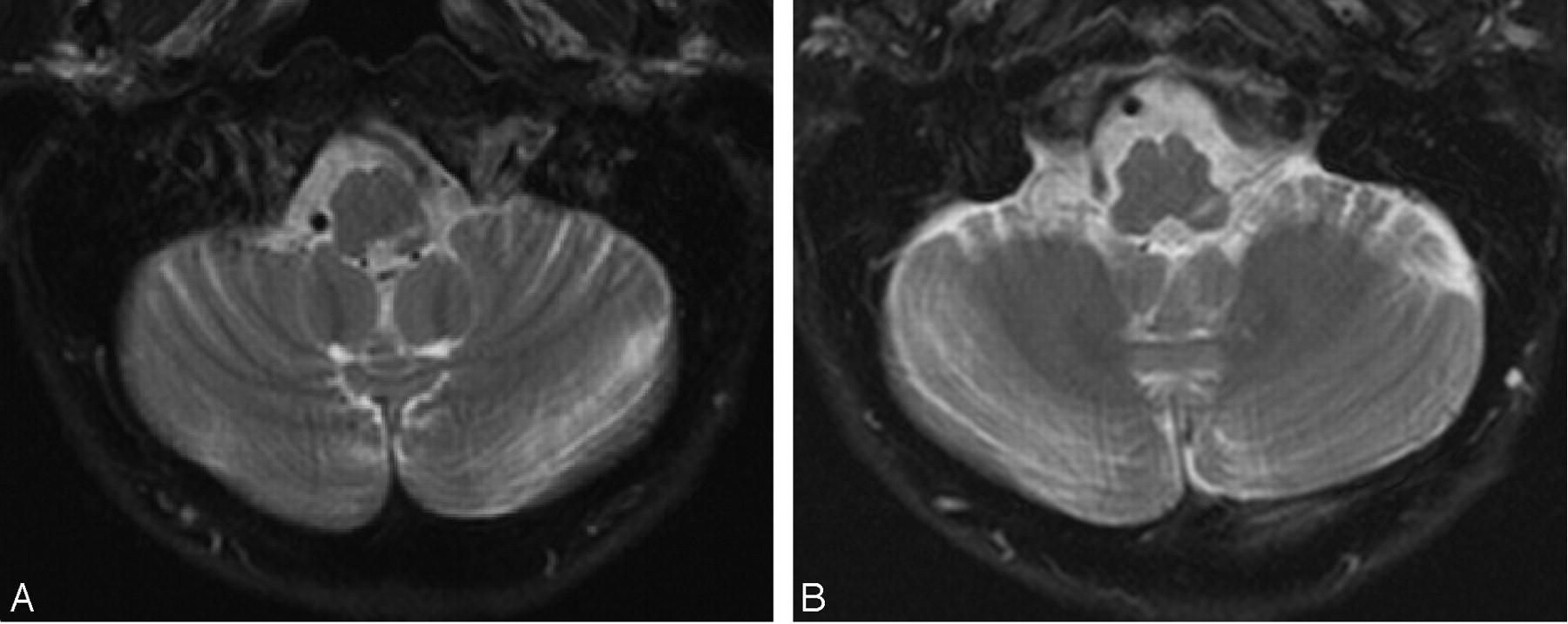
Seven weeks after the onset of symptoms, we performed high-resolution brain MR imaging to evaluate the trigeminal nerve pathway. MR demonstrated linear increased signal intensity on T2 sequences in the lateral left medulla in the left spinotrigeminal nucleus and tract (Fig 1A,-B) and left solitary nucleus. Diffusion-weighted imaging (DWI) was normal, and there was no enhancement with gadolinium. Trigeminal and glossopharyngeal nerve signal intensities were normal and without enhancement, and there was no vascular compression of the trigeminal nerve roots at the pontine nerve root entry zone on coronal 3D-constructive interference in steady state (3D-CISS; Fig 1C). There was no evidence of dissection on MR angiography (MRA), and the left posterior inferior cerebellar artery was patent. These findings were consistent with a chronic left LMI, presumably secondary to small vessel ischemia. Although the outside MR imaging study performed 1 week after the onset of symptoms was normal by report, these images were not available for our review. In conjunction with the laterality and sudden onset of symptoms and involvement of the trigeminal, solitary, and ambiguus nuclei by the infarction, we infer that these imaging findings are coincident with the patient’s symptom onset.


T2-weighted axial view images (A and B) show linear increased signal intensity in the left lateral medulla in the left spinotrigeminal nucleus and tract and left solitary nucleus. A coronal 3D-CISS image (C) demonstrates no compression of the trigeminal nerve at the pontine nerve root entry zone.
The patient was treated with clonazepam 0.5 mg nightly, and although she continued to experience mild attacks of trigeminal and glossopharyngeal-distribution pain, 3 weeks later her symptoms had significantly improved.
Discussion
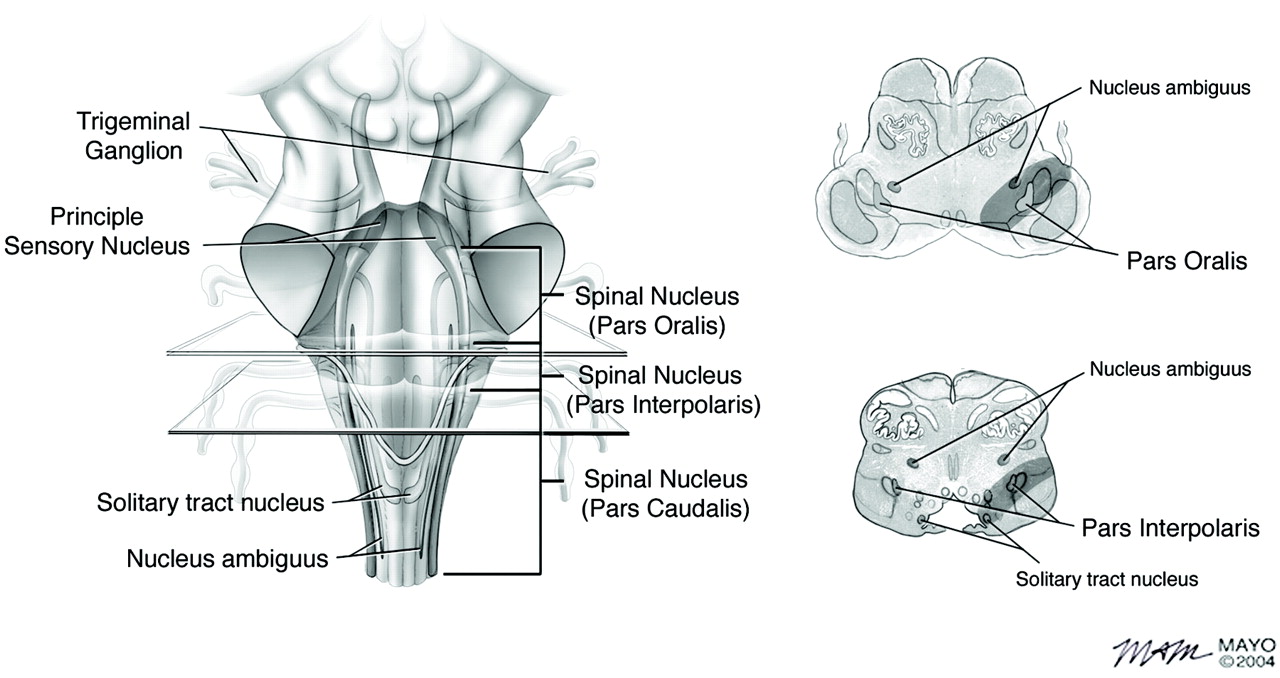
TN is an uncommon pain disorder, with an incidence of approximately 15,000 new cases per year.3 Concurrent ipsilateral TN and GPN is rare, representing 10.0% to 46.7% of GPN cases but only 0.3% to 0.5% of TN cases.4 TN demonstrates a 3:2 female predominance. The average age at onset is the sixth to seventh decades, although symptomatic TN can present in younger populations. Most TN cases involve both the maxillary and mandibular divisions simultaneously, although TN can affect any division alone or in combination. GPN, also termed vagoglossopharyngeal neuralgia because of pain distribution along vagal sensory nerves, can be associated with bradycardia, asystole, mental confusion, syncope, and convulsions.5 GPN presents as recurrent tongue, tonsil, throat, and ear pain with a comparable time course to TN and also with detectable triggers including swallowing and talking.6 Symptomatic GPN can be caused by oropharyngeal cancer, retropharyngeal infection or hematoma, and vascular compression.7 Simultaneous TN and GPN suggest a structural lesion in an area that could capture both trigeminal and glossopharyngeal nerve pathways. From an anatomic perspective, the spinotrigeminal nucleus and tract (CN V), the solitary nucleus (CN VII, IX, and X) and the nucleus ambiguus (CN IX and X) are in close proximity in the medulla (Fig 2).

Coronal and axial sketches of the medulla, which correspond to the medullary regions seen on the T2-weighted axial images in Fig 1, demonstrate the anatomical proximity of the spinotrigeminal nucleus and tract to the solitary nucleus and nucleus ambiguus.
The trigeminal nerve sensory afferents for discriminative touch exit the semilunar or Gasserian ganglion in the Meckel cave, traverse the prepontine cistern, and enter the brain stem at the lateral midpons, terminating in the principal sensory nucleus in the dorsolateral pontine tegmentum. Pain, temperature, and light touch sensory afferents enter the lateral midpons and travel caudally to form the spinal trigeminal tract. A small number of facial, glossopharyngeal, and vagus nerve fibers also travel within the tract. The tract fibers terminate in the adjacent spinal trigeminal nucleus and in the reticular formation medially. The spinal trigeminal nucleus extends from the lateral midpons to the cervical spinal cord at the level of C3. This nucleus is composed of pars oralis, pars interpolaris, and pars caudalis. Pars oralis extends from the principal sensory nucleus to the inferior olivary nucleus and receives epicritic pathways from the face for light touch. Pars interpolaris extends from the inferior olivary nucleus to the pyramidal decussation, receiving fibers for touch and temperature. Pars caudalis extends from the pyramidal decussation to the C3 cervical spinal cord and receives protopathic fibers for pain and temperature. The nucleus ambiguus travels adjacent to the pars interpolaris and caudalis, housing the origins of glossopharyngeal, vagus, and accessory motor fibers, providing innervations to pharyngeal and laryngeal muscles, trapezius, and sternocleidomastoid. The solitary nucleus receives fibers from the glossopharyngeal and vagus nerves and the nervus intermedius. Its upper part receives gustatory fibers from the glossopharyngeal nerve and nervus intermedius. Its mid and lower portions receive fibers from visceral organs and blood vessels (Fig 2).8
MR is the imaging technique of choice in TN evaluation, with demonstration of the trigeminal nerve and nuclei throughout their entire course. MR imaging and MRA are best used when there are other neurologic deficits, as in this case with associated GPN, symptom progression, symptoms for less than 1 year, and a younger age at onset. Isolated TN symptoms without other physical findings commonly show negative MR imaging/MRA.9 The most frequent location of TN-related pathology is of the cisternal portion of the nerve at the pontine root entry zone, though the cavernous and extracranial portions can also be involved.
Infarction leading to TN is usually found in the principle sensory nucleus in the pons. Nerve root entry zone infarction has also been reported as a cause of TN.10 One report11 describes LMI as a cause of TN but without other associated cranial nerve findings. Concurrent TN and GPN occurring because of LMI have, to our knowledge, never been described previously.
DWI and apparent diffusion coefficient (ADC) MR imaging are the most effective sequences for revealing infarction in its earliest phases, whereas T2 and fluid-attenuated inversion recovery (FLAIR) sequences do not show changes of ischemia for several hours after symptom onset. Integrating data from DWI, ADC, T2, and FLAIR images, however, is useful in more accurately defining stroke age.12
Other structural lesions associated with TN can include compression from adjacent arteries or veins, basilar aneurysm, multiple sclerosis, and cerebellopontine angle tumor. Vascular compression, most commonly arising from the superior cerebellar artery,3 is responsible for approximately 80% to 90% of TN1 and is also likely to play a role in some cases of GPN. MR imaging and MRA are useful in illustrating the proximity of compressive vessel or aneurysm and nerve. MR 3D-CISS or 3D-fast inflow with steady state precession can also clearly define a culprit vessel, with positive correlation to intraoperative pathology.13 Multiple sclerosis leading to TN and GPN most commonly involves the dorsolateral pons but can also involve the trigeminal nerve at the root entry zone. MR imaging typically demonstrates multiple focal areas of plaquelike increased signal intensity consistent with demyelinating disease.14 Neoplastic processes, which can cause compression of the trigeminal nerve at the pontine nerve root entry zone, are easily detected with gadolinium-enhanced MR imaging.
Current treatment options for TN and GPN include both medical and surgical therapy. General practice is to attempt to resolve patient symptoms by using drug therapy before resorting to surgery. Drug therapies typically attain effect by reducing trigeminal/glossopharyngeal response to sensory stimulation. Good response rates have been achieved with antiseizure medications. If medical therapy fails to resolve the patient’s symptoms or if they become drug intolerant, there are several surgical options, including radiofrequency thermocoagulation and microvascular decompression, which are the 2 most common procedures performed. Others are gamma knife radiosurgery, trigeminal ganglion electrical stimulation, percutaneous balloon compression, glycerol rhizotomy, and extracranial peripheral denervation. Important factors to consider for each procedure are time until pain relief, length of response, recurrence rate, safety, side effects, availability, and cost, which vary for each procedure.3 Despite poor response to oxcarbazepine and gabapentin, our patient is currently responding to clonazepam, foregoing the need for surgical management at this time.
TN and concurrent GPN presenting as a consequence of lateral medullary vascular compromise is unusual, especially in light of the relative lack of associated symptoms and signs. Isolated TN is more readily seen with lesions involving the cisternal portion or root entry zone of the nerve. When a structural lesion is suspected, or if there is concurrent involvement of other cranial nerves, as in this case, advanced MR imaging plays an important role, because lack of DWI and gradient echo modalities can lead to false-negatives. 3D-CISS images of the pons are essential to evaluate for compression of the trigeminal nerve, the most common cause of TN. When a cause cannot be identified at the root entry zone, we recommend imaging the entire extent of the trigeminal and glossopharyngeal neural pathways into the upper cervical spinal cord to identify structural causes of TN and GPN.
References
- Received February 28, 2005.
- Accepted after revision May 9, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.