
Abstract
SUMMARY: We report the case of a 1 -year-old female child, who developed symptomatic hemorrhage from major aorto-pulmonary collaterals after surgery for Tetrology of Fallot. During the course of embolization of the aorto-pulmonary collaterals, we discovered the presence of direct origin of the left internal and external carotid arteries from the aortic arch. Further, there was cervical origin of right subclavian artery. We discuss the clinical significance and potential embryological mechanism in development of this anomaly.
-year-old female child, who developed symptomatic hemorrhage from major aorto-pulmonary collaterals after surgery for Tetrology of Fallot. During the course of embolization of the aorto-pulmonary collaterals, we discovered the presence of direct origin of the left internal and external carotid arteries from the aortic arch. Further, there was cervical origin of right subclavian artery. We discuss the clinical significance and potential embryological mechanism in development of this anomaly.
Absence of the common carotid artery is an extremely rare anomaly. Fewer than 25 cases have been reported in the literature, and only 6 cases have been characterized by angiographic studies.1 Likewise, cervical origin of the right subclavian artery (CORSA) is a rare anomaly. CORSA is defined as an abnormally high origin of the right subclavian artery from the common carotid artery close to the bifurcation of the internal and external carotid arteries.2 The identification of this anomaly has been given importance recently, in that the presence of this entity has been described as a specific marker for the presence of monosomy 22q11.2 To the best of our knowledge, the coexistence of these rare anomalies has not been described before. We report the angiographic findings in a child in whom the anomalies were discovered during embolization of bleeding major aortopulmonary collateral arteries (MAPCAs). The presence of these anomalies proved detrimental to the outcome of the procedure.
Case Report
A 1.5-year-old girl was brought to our institute with history of breathlessness and cyanosis since 3 months of age. Clinical examination revealed central cyanosis and ejection systolic murmur in the pulmonary area. Echocardiographic findings were suggestive of tetralogy of Fallot with pulmonary artery stenosis. A left-sided Blalock-Taussig (BT) shunt was planned. Blalock and Taussig developed their pioneering operation for cyanotic children in 1945, and it has continued to be a very successful operation to this day. In the beginning, the artery to the arm (subclavian) was stitched directly to the pulmonary artery, which allowed extra blood from the aorta (body artery) to pass into the lungs and receive oxygen. This is called a classic BT shunt. Because the blood supply to the arm is reduced, some children experienced problems, so a later development was the modified BT shunt, in which a tube made of Gore-Tex is stitched between the arm and lung arteries. In view of the intraoperative finding of good pulmonary artery anatomy, however, biventricular repair was performed.
Approximately 12 hours after the surgery, the child exhibited a progressive decline in the level of blood oxygen saturation. Auscultation of the chest revealed coarse crepitations. Suction of the endotracheal tube revealed blood-stained secretions. Intrapulmonary hemorrhage due to bleeding MAPCAs was suspected, and the child was taken for angiography and embolization.
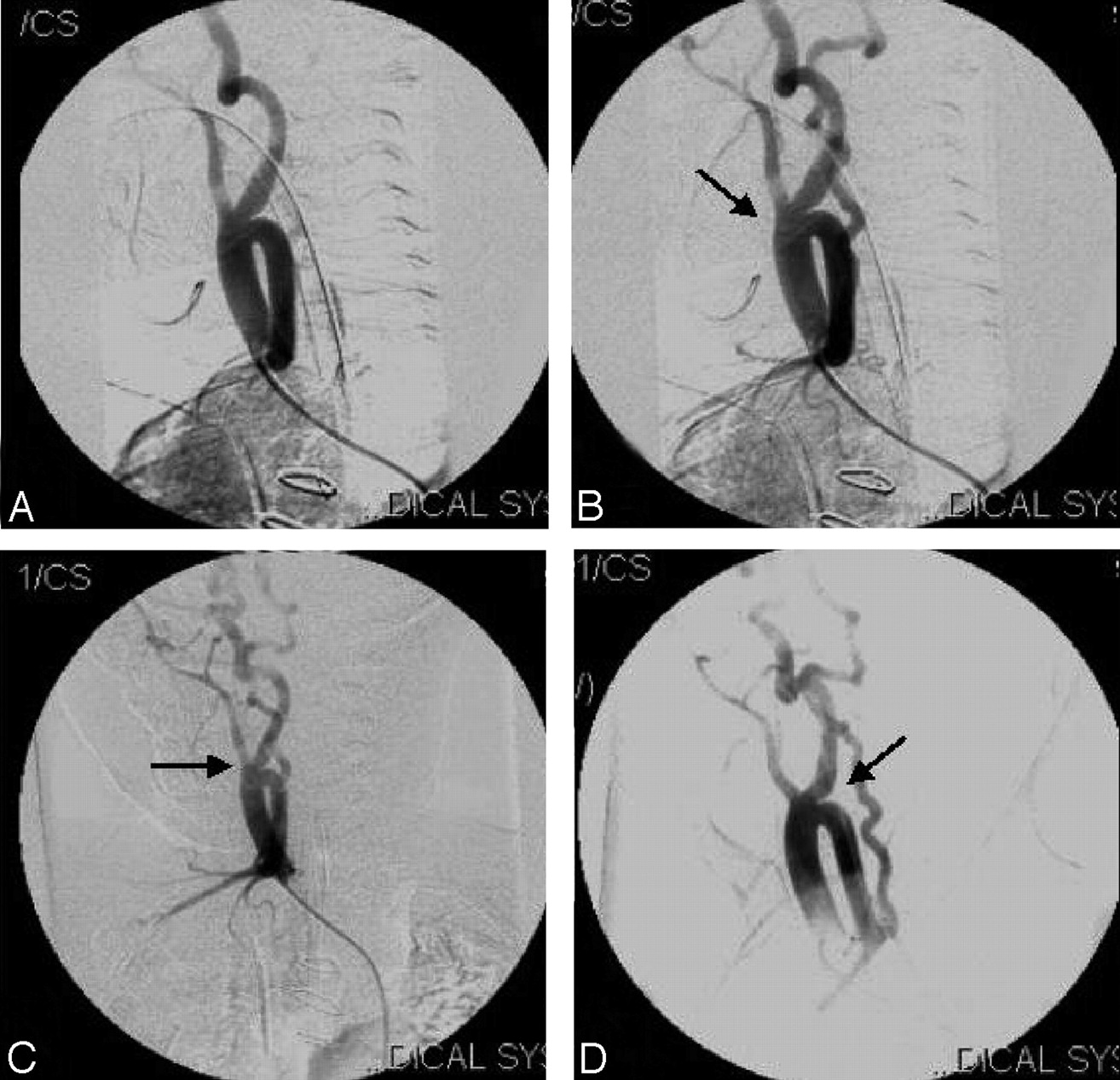
An aortogram revealed a left-sided aortic arch, with the brachiocephalic artery as the first vessel originating from it (Fig. 1). The brachiocephalic artery extended superiorly into the neck and trifurcated at the level of the hyoid bone into the external and internal carotid arteries and the right subclavian artery (Fig. 2). The right subclavian artery coursed posteriorly in its initial segment, inferiorly, and then laterally into the arm (Fig 3). The origin and course of the right vertebral artery were normal (Fig 4). The second vessel originating from the aortic arch was the left external carotid artery, which was closely followed by the origin of the left internal carotid artery (Fig 1B). Attempts at selective catheterization of the origins of internal and external carotid arteries to study the intracranial circulation were unsuccessful, because of loops at the origin of these vessels, and were abandoned to limit the volume of contrast medium used during the procedure. The origin and course of the left subclavian artery were normal (Fig 5). MAPACs were noted, supplied by the left thyrocervical trunk, right bronchial artery, and the right thyrocervical trunk. The right bronchial artery was initially catheterized by using a 4F Judkin right coronary catheter (Cordis, Miami Lakes, Fla) and 250 to 355-μm polyvinyl alcohol (Target Therapeutics, Fremont, Calif) particles were injected to obliterate the collaterals (Fig 6). Thereafter, the left thyrocervical trunk (Fig 7) was cannulated with a 3F catheter (Terumo Corporation, Tokyo, Japan) and embolized with 250 to 355-μm polyvinyl alcohol particles (Target Therapeutics). Prolonged attempts at catheterization of the right thyrocervical trunk were unsuccessful, because the guide catheter could not be negotiated past the brachiocephalic trifurcation, into the descending segment of the right subclavian artery. The procedure had to be terminated even though there was residual opacification of MAPCAs. During the course of the procedure, the partial pressure of oxygen in arterial blood (Pao2) improved from 40 mm Hg to 60.5 mm Hg.

A, Arch aortogram shows the origin of brachiocephalic artery and other vessels. B, Little distal injection in the arch shows the separate origins of external carotid artery, internal carotid artery and left subclavian artery. Note the loops at the origin of both the external and internal carotid arteries (thick arrow).

A–D, Right brachiocephalic artery injection with early (A) and late arterial phases (B–D) on different angulations show the trifurcation of brachiocephalic artery into right subclavian, right internal and external carotid arteries (thick arrows, B–D). Note the CORSA and the vessel coursing downward and laterally into the arm (B and D).

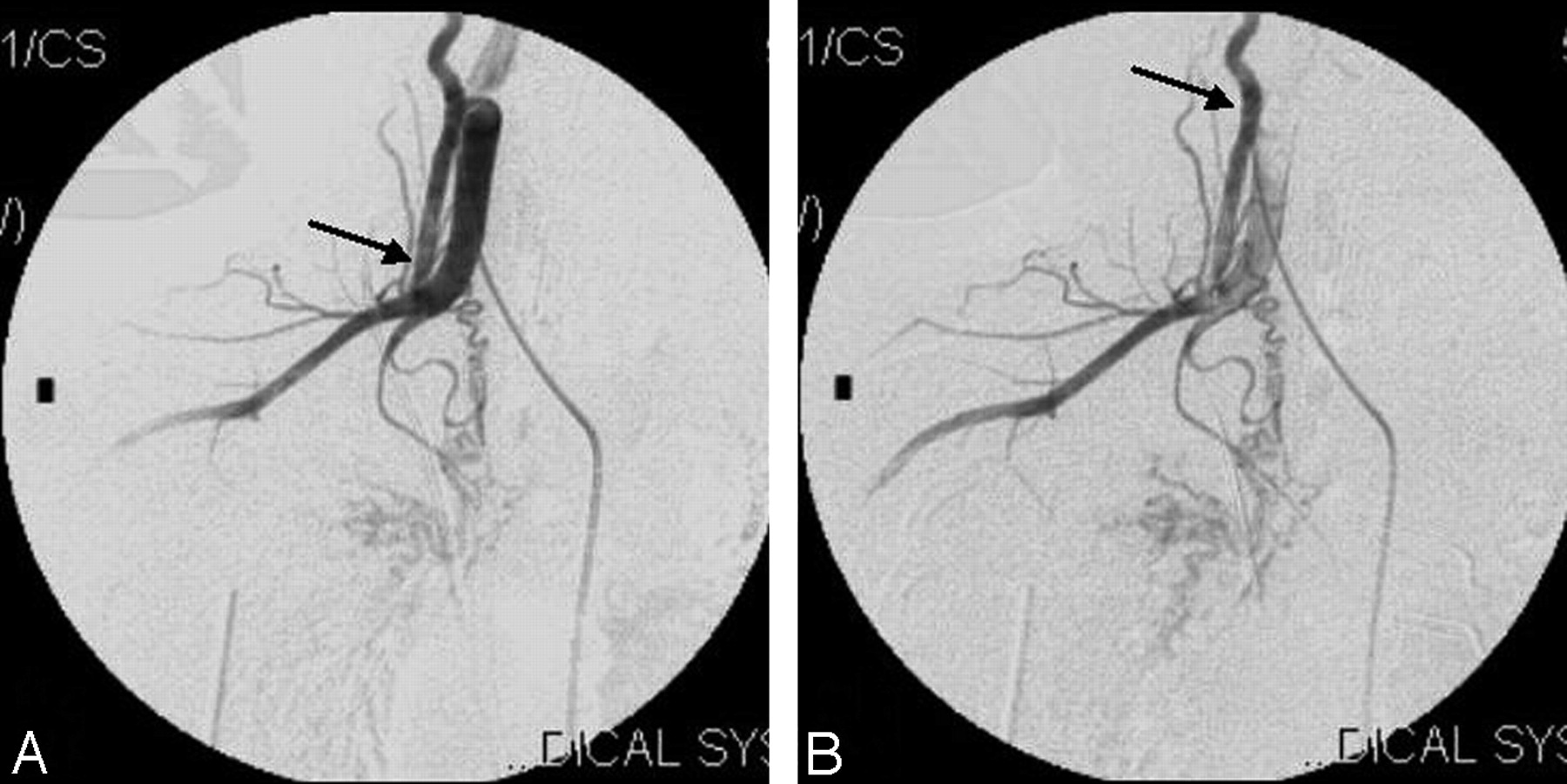
A, Selective injection of the right subclavian artery shows its cervical origin and the vessel coursing inferolaterally (arrow) in the neck and then to the right arm.
B, The right thyrocervical artery (thin arrow) is seen to supply major pulmonary collaterals (MAPCA). Note the abnormal blush in lung parenchyma (thick arrow).

Right subclavian artery injection, (A) early and (B) late phases, showing the normal origin of the right vertebral artery (arrows).

A, Injection at the origin of the left subclavian artery shows its normal origin and course to the left arm (arrow).
B, Late phase of the same injection shows the MAPCA from right thyrocervical artery (thin arrow).

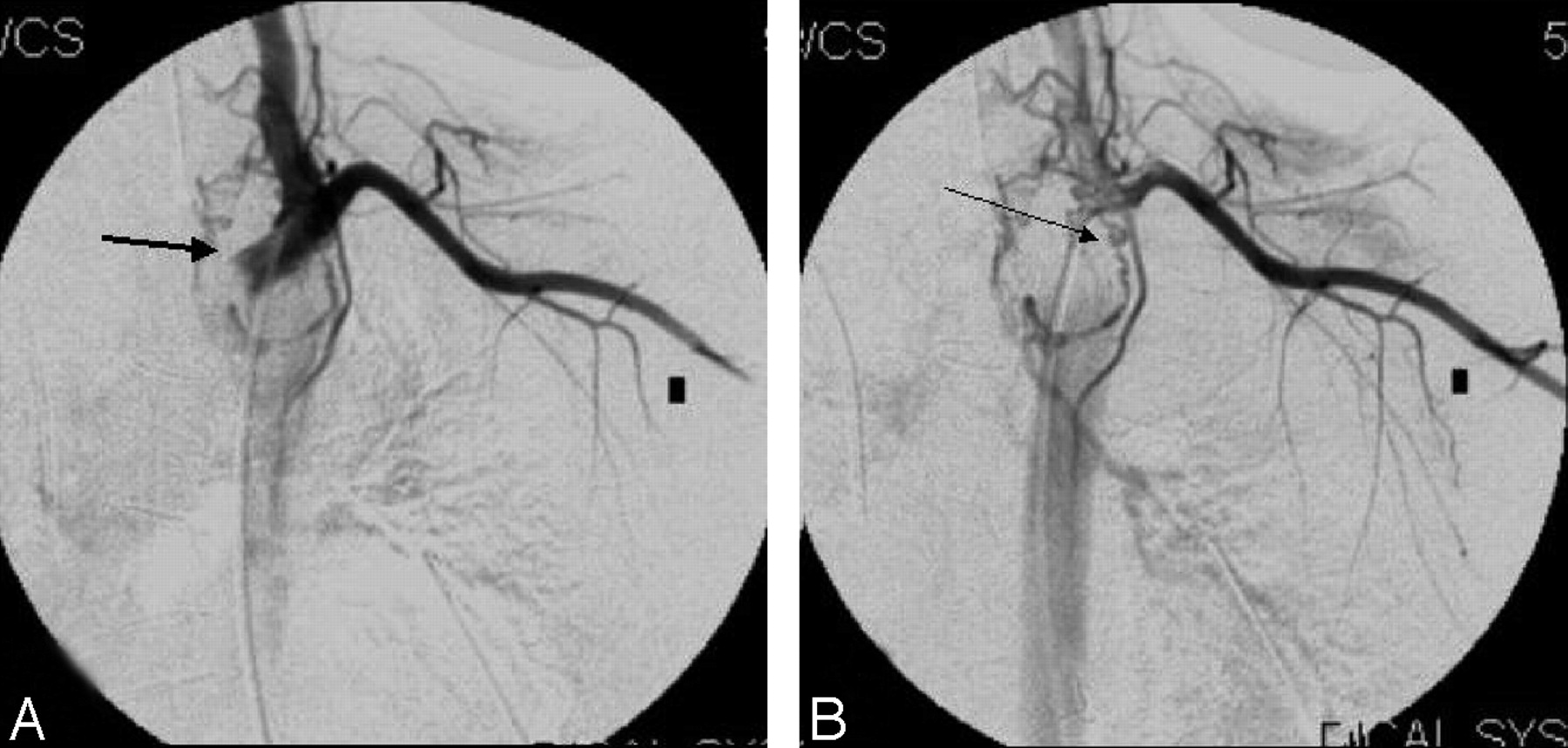
A, Right bronchial artery injection shows the abnormal blush (arrow).
B, Postembolization angiogram of right bronchial artery (arrow) shows the complete disappearance of the abnormal blush.

Pre-embolization (A, arrow) and postembolization (B) angiograms of left thyrocervical trunk supplying the pulmonary circulation.
During the postprocedural period, the child was well hydrated. Despite all precautionary measures, approximately 6 hours after the procedure, urine output progressively decreased and she became anuric. Peritoneal dialysis was instituted immediately. The subsequent period was characterized by progressive deterioration of the oxygen saturation levels. Approximately 24 hours after the procedure, reappearance of coarse crepitations and blood-stained secretions in the airway indicated ongoing hemorrhage within the lung. Despite all medical measures, the child continued to deteriorate and died 3 days later.
Discussion
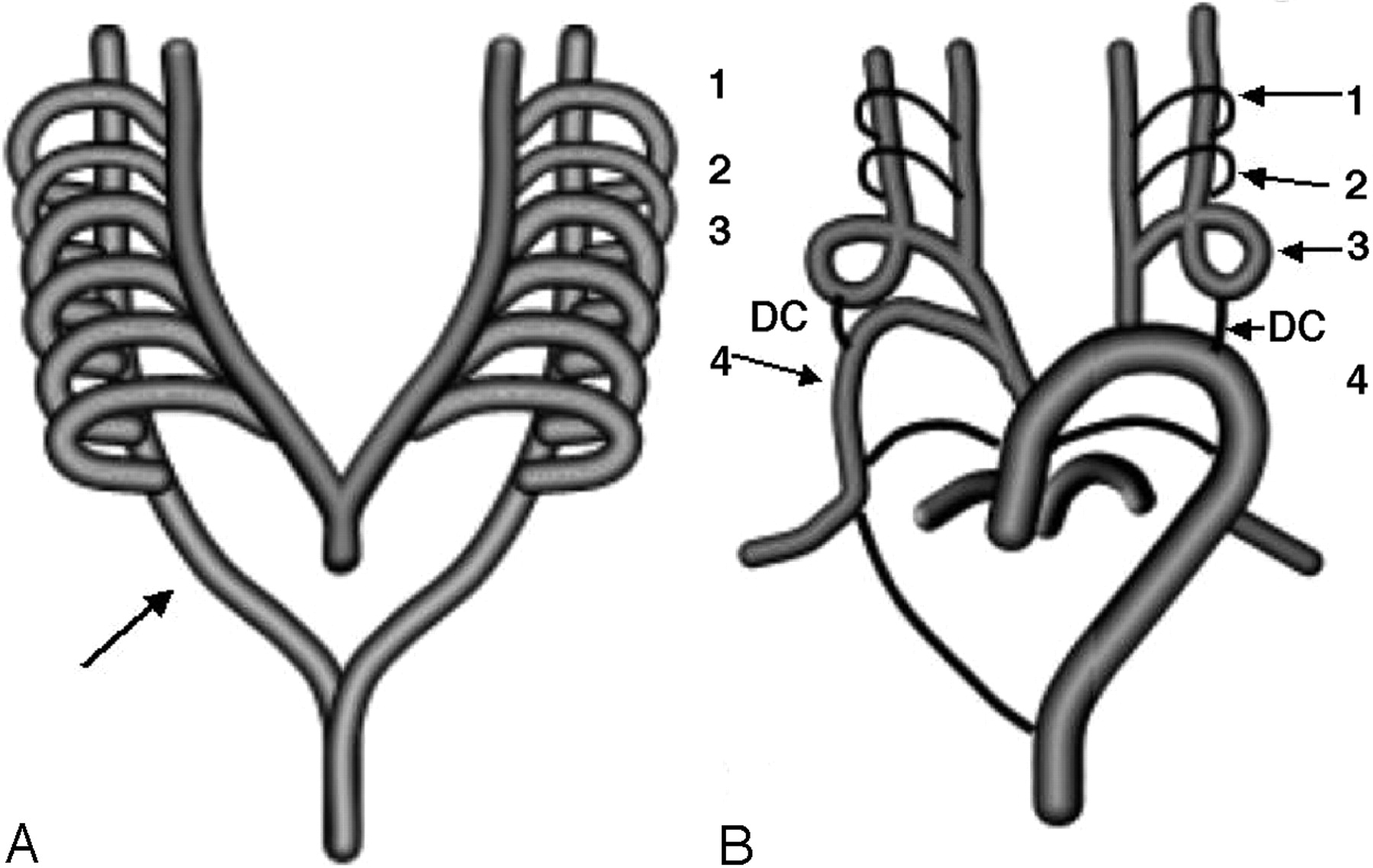
Congenital anomalies of the craniocerebral circulation are encountered along with congenital malformations of the heart. Embryogenesis of these malformations can be best understood in correlation to normal development of aortic and supra-aortic vessels (Fig 8A, -B). Abnormal embryogenesis can be obtained by analysis of these anomalies. Absence of the common carotid artery has been described to occur either because of persistence of ductus caroticus with regression of third arch or because of regression of the fourth arch. When the absence of common carotid artery occurs on the right side, the internal and external carotid arteries arise from the right subclavian artery. When this anomaly occurs on the left side, the internal and external carotid arteries arise from the aortic arch (Fig 9).1 This anomaly has been described in association with other malformations such as cervical aortic arch, double aortic arch, right-sided aortic arch with aberrant left subclavian artery, persistent trigeminal artery, and type II proatlantal artery.1,3

A, Normal development of aortic arch. Six aortic arches connecting the ventral to the dorsal aortas are seen (arrow).
B, Normal evolution of the arches: DC, ductus caroticus; 1 to 4, aortic arches (arrows). Fourth arch and the dorsal aorta on the right side form the normal subclavian artery (arrow). Third arch along with parts of the ventral and dorsal aorta form the internal and external carotid arteries. Fifth arches involute, and the sixth form the pulmonary arteries.

The right ductus caroticus (arrow), the right seventh intersegmental artery and the right dorsal aorta below the level of the third arch form the right subclavian artery arising from right common carotid artery. Persistence of ductus caroticus with regression of third arch or fourth arch causes the internal and external carotid arteries to arise from the aortic arch on the left side. DC, ductus caroticus; 1 to 4, aortic arches (arrows).
Kutsche and Van Mierop4 described CORSA in 1984. They found this anomaly in 4 of 21 infants (19%) studied for aortic arch interruption. The origin of the vessel was seen along with the origins of the internal and external carotid arteries as a trifurcation, at the level of the thyroid gland. It then descended down the neck to enter the right arm. The right recurrent laryngeal nerve was seen to course around the origin of the right subclavian artery, much higher than normal. The pathogenesis of CORSA can be explained by impairment of fourth aortic arch development, before the involution of the right ductus caroticus (segment of the dorsal aorta between the third and fourth arches). The right ductus caroticus, which normally involutes at the 14-mm crown-rump length, is retained and forms the initial segment of the right subclavian artery at its origin from the common carotid bifurcation. The seventh intersegmental artery and the dorsal aorta below the level of the third arch form the rest of the subclavian artery.
In 2002, Rauch et al2 described the frequency of the anomalies of subclavian arteries in 136 patients with conotruncal malformations. They found CORSA in 11 of the 37 patients who had anomalies of origin of the subclavian arteries. The associated cardiovascular anomalies in these cases included interruption of aortic arch in 6 patients, pulmonary atresia with ventricular septal defect in 4 patients, and tetralogy of Fallot in one patient. Cytogenetic analysis revealed microdeletion in the long arm of chromosome 22 in the region 22q11 in all patients with CORSA. The authors reported that detection of CORSA could represent a specific marker for monosomy 22q11. This is serious disorder and can be associated with other serious cardiac anomalies. Molecular cytogenetic analyses have demonstrated that deletion of chromosomal region 22q11 is closely related to conotruncal cardiac defects such as truncus arteriosus, tetralogy of Fallot, pulmonary atresia with ventricular septal defect, and interrupted aortic arch.2 Greil et al5 recently reported a case of CORSA and demonstrated in their patient that CORSA is highly specific for 22q11 syndromes.
The abnormal anatomy in our case may be explained by regression of the right fourth aortic arch and the left third aortic arch. The persistent ductus caroticus on both sides may have participated in the formation of the proximal subclavian artery on right side and proximal internal carotid artery on the left side. Cytogenetic analyses could not be performed on the child. Autopsy would have given additional information on the exact cause of death and the nature of any other associated congenital anomalism, but the parents of the child did not consent.
The presence of such anomalous connections is usually discovered as an incidental finding when imaging studies are performed for other clinical entities. Cakirer et al6 have reported a patient with absent common carotid artery, which was diagnosed on MR angiogram. The anomalies themselves may be responsible for atypical presentation of neurologic illnesses. Jerius et al7 have described a patient without a right common carotid artery in whom superimposition of significant atherosclerotic disease over the congenital anomaly resulted in severe vertebrobasilar ischemia. In our patient, however, the unfavorable anatomy associated with the anomaly was responsible for prolonging the interventional procedure, with an attendant increase in the volume of contrast medium that was used. The abrupt retrograde course of the subclavian artery within the neck did not permit the passage of the guiding catheter and any other suitable catheter distally enough to support the microcatheter to catheterize the MAPCAs supplied by the right thyrocervical artery. Use of contrast was minimized to 4 mL per kg of body weight. The patient, however, developed urinary shutdown and continuing hemorrhage from the incompletely embolized MAPCAs that were responsible for her poor outcome. Pulmonary artery stenosis with tetralogy of Fallot resulted in MAPCAs in this patient. Suboptimal embolization could have resulted in continued bleeding from MAPCAs and the child’s eventual clinical deterioration.
References
- Received January 11, 2005.
- Accepted after revision May 9, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Ruptured anterior communicating artery aneurysm associated with internal carotid artery absence
- Republished: A rare case of absent left common carotid artery with bovine origin of the left external carotid artery
- A rare case of absent left common carotid artery with bovine origin of the left external carotid artery