
Article Figures & Data
Figures
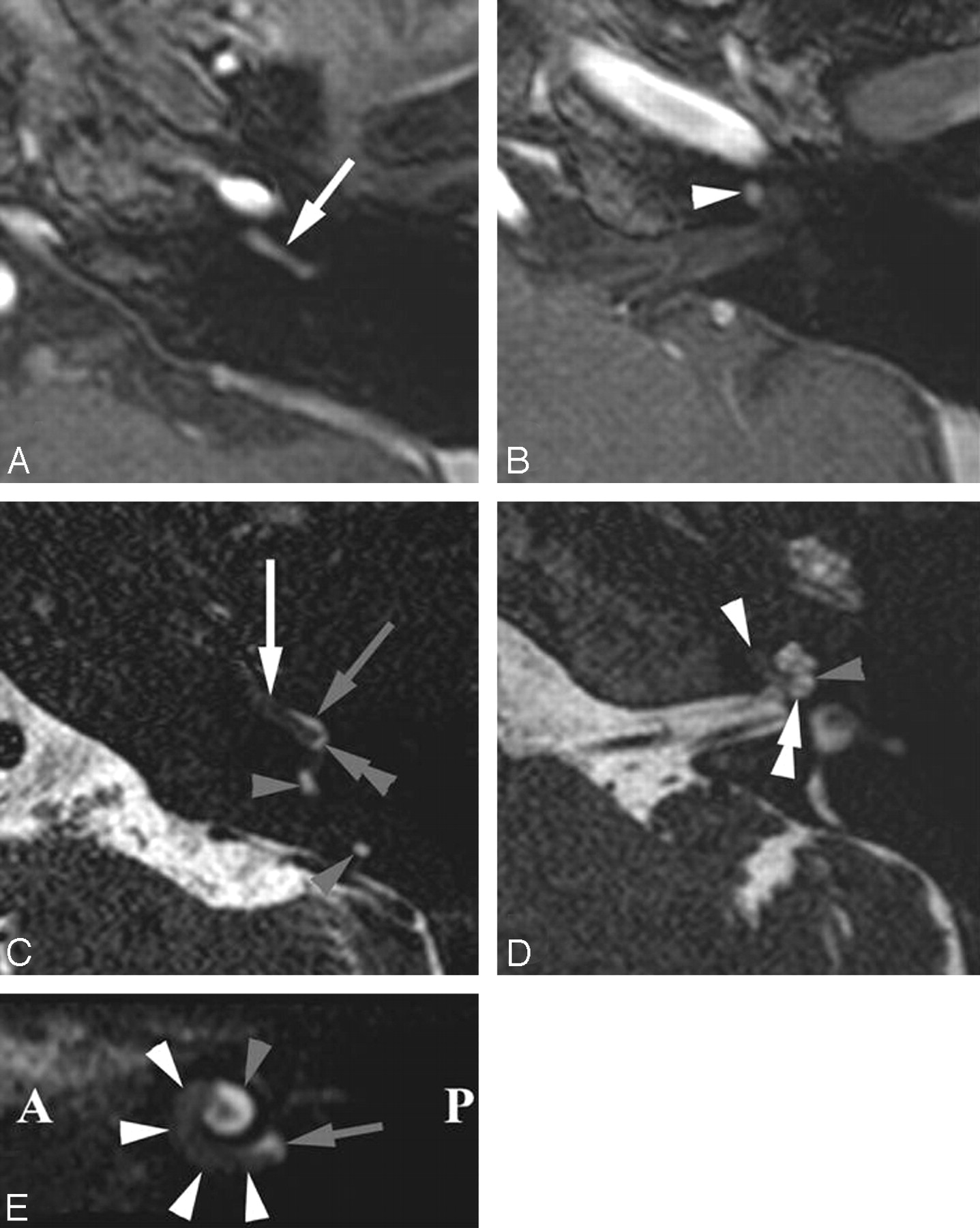
- Fig 1.
Intracochlear schwannoma in the BT and anterior SecT of the left cochlea. Axial Gd-enhanced T1-weighted images (A and B) and heavily T2-weighted DRIVE images (C and D) through the BT (A and C) and ST (B and D) and parasagittal DRIVE reconstruction (E). A, Enhancing schwannoma in BT (white arrow). B, Extending into anterior part of SecT (white arrowhead). C, Schwannoma anteriorly in both scalae of the BT (white arrow) and posteriorly in the ST of the BT (double gray arrowhead). Normal fluid in posterior SV (gray arrow): schwannoma occupies ST more than SV. Normal fluid in posterior semicircular duct (gray arrowheads). D, Anterior parts of both scalae of SecT were occupied (white arrowhead). Normal fluid in SV (gray arrowhead) and ST (double white arrowhead) of posterior SecT. E, Schwannoma in BT and anterior part of SecT (white arrowheads). Fluid signal intensity still present near the round window (gray arrow) and posterior part of ST (gray arrowhead). A indicates anterior; P, posterior; SecT, second turn of cochlea; BT, basal turn of cochlea; ST, scala tympani; SV, scala vestibuli.
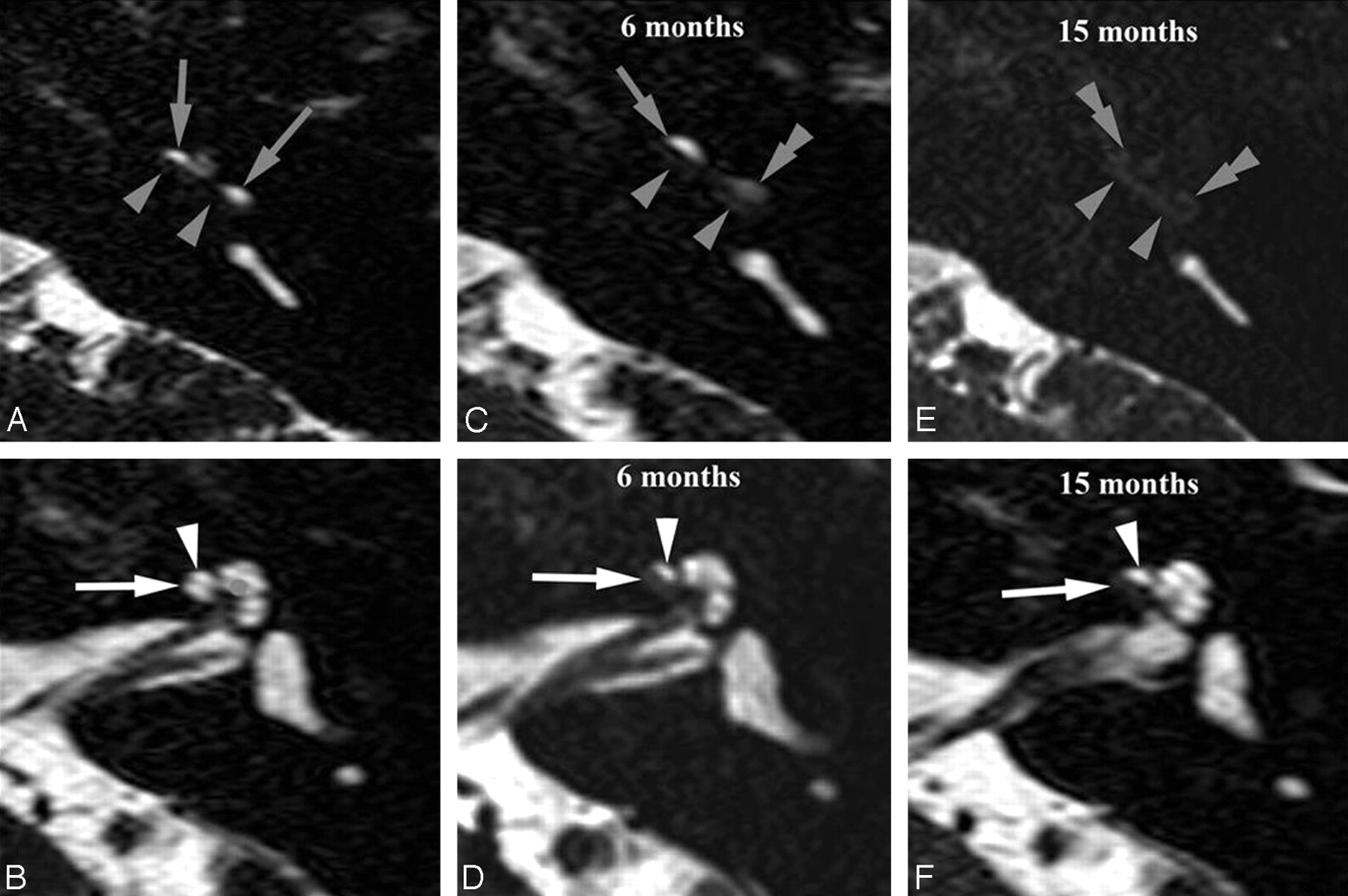
- Fig 2.
Intracochlear schwannoma gradually occupying entire ST and growing into the SV. Axial heavily T2-weighted DRIVE images through the basal turn (BT) (A, C, and E) and second turn (SecT) (B, D, and F). A and B, At presentation, obliteration of entire ST of the BT (gray arrowheads). Normal signal intensity inside SV of BT (gray arrows). Normal hyperintense fluid signal intensity inside SV (white arrowhead) and ST (white arrow) of the SecT. C and D, Six months later, loss of fluid signal intensity in SV posteriorly in BT (double gray arrowhead), confirming extension from ST (gray arrowheads) into the posterior SV. Anterior part of SV was still open (gray arrow). Invasion of the ST in anterior part of SecT (white arrow), confirming further growth inside the ST. E and F, After 15 months, further growth inside SV of BT (double gray arrowheads). ST of BT is still completely obliterated (gray arrowheads). No further growth in ST of SecT (white arrow). SV remained open (white arrowhead).
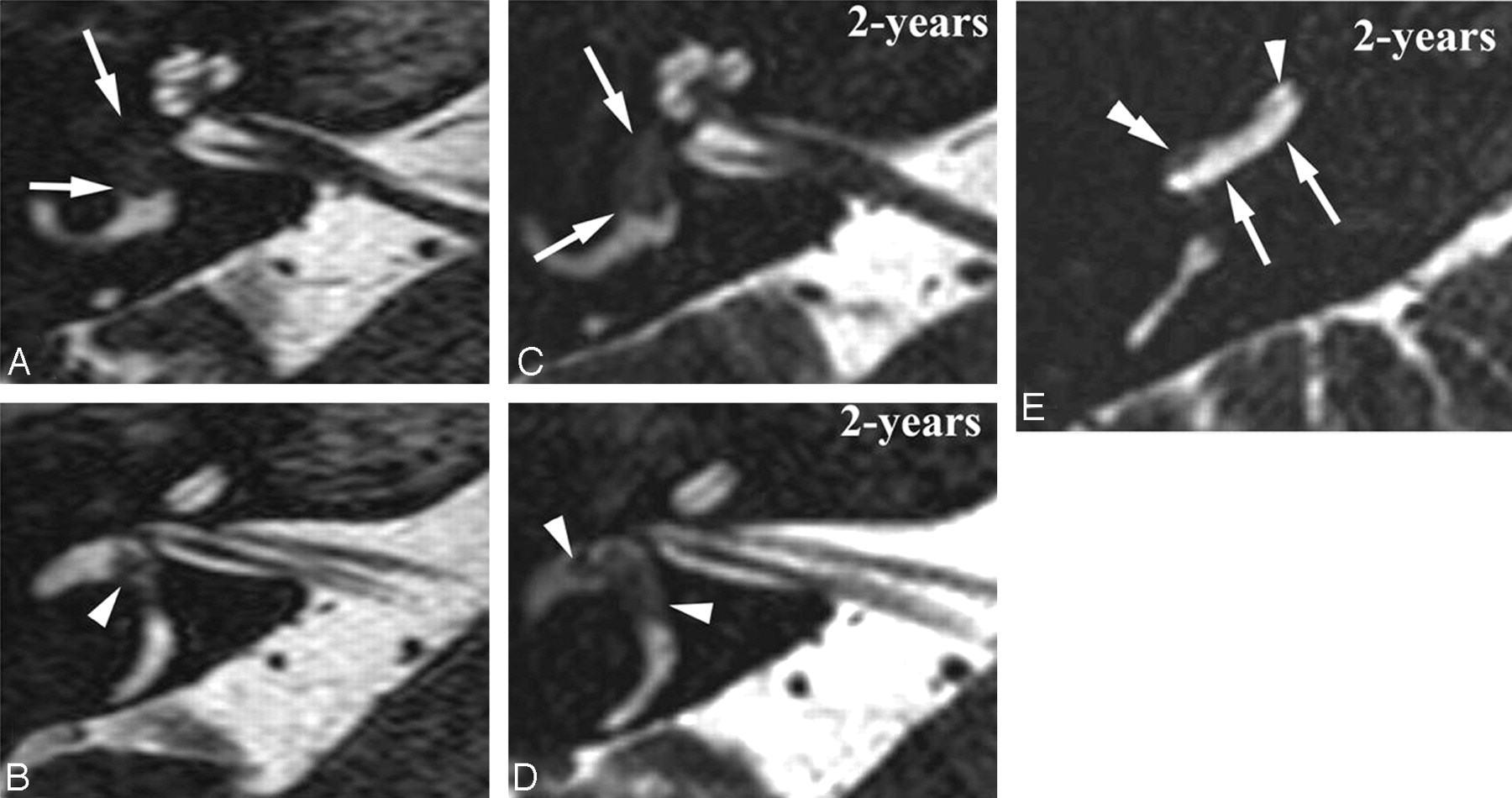
- Fig 3.
Intravestibular schwannoma growing inside the right vestibular system and into the basal turn (BT). Axial DRIVE images through the midcochlea (A and C) and upper part of the SecT (B and D) and axial DRIVE image through the BT. A and B, Intravestibular schwannoma inside the anterior vestibule (white arrows) and ampulla of the lateral SCC (white arrowhead). C and D, 2 years later, schwannoma extended more posteriorly in the vestibule (white arrows) and occupied a larger part of the ampulla of the lateral SCC (white arrowheads). E, The schwannoma also grew back into the cochlea. Because of the open anatomic connection between the saccular perilymphatic space and perilymph inside the SV, the schwannoma will first grow into the SV of the posterior BT (double white arrowhead). Normal signal intensity still present in anterior part of SV (white arrowhead) and entire ST (white arrows).
- Fig 4.
Intracochlear schwannoma with a 5-year MR FU showing growth into the vestibule and IAC. Axial Gd-enhanced T1-weighted images through the basal turn (BT) (A, D, G, and J), second turn (SecT), and apical turn (AT) (B, E, H, and K) and the upper part of the SecT and vestibule (C, F, I, and L). A–C, At presentation: enhancing schwannoma anteriorly in BT (white arrow) and SecT (white arrowhead). D–F, 3-years later, growth into posterior part of both BT (white arrow) and ST (white arrowheads) and into anteroinferior part of the vestibule (gray arrow). Subtle enhancement near the IAC fundus (black arrow) suspicious for extension into the IAC. G–I, After 4-years, enhancement at IAC fundus became nodular (black arrow), confirming growth into the IAC. Enhancement in AT (gray arrowhead) and the anteroinferior part (gray arrows) and also in the superior part of the vestibule (double gray arrowhead), indicating further growth. J–L, After 5 years, further growth with complete enhancement of AT (gray arrowheads), larger extension in IAC (black arrow), and involvement of posterior-inferior (gray arrows) and superior parts (double gray arrowheads) of the vestibule.
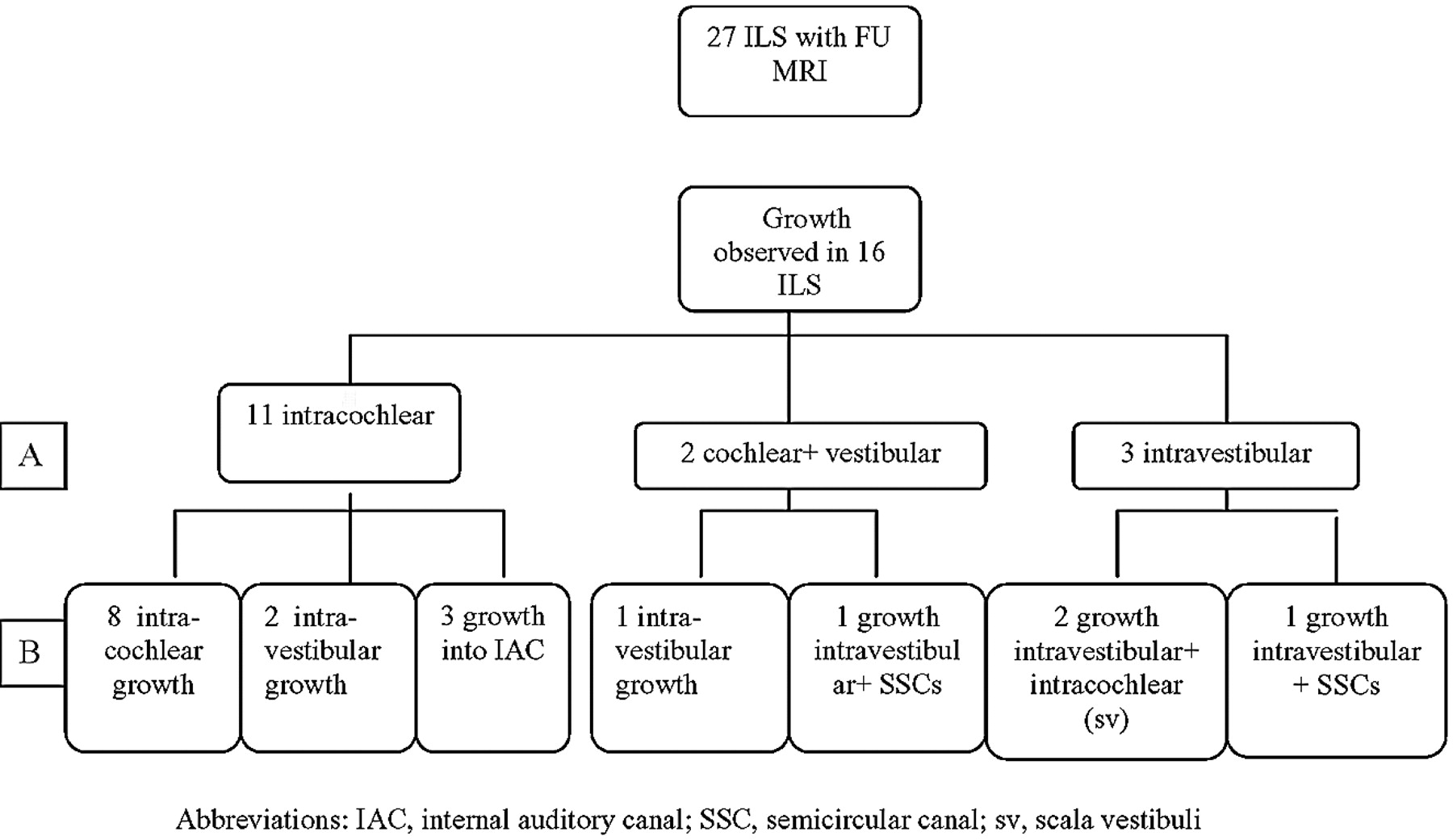
- Fig 5.
Flow chart illustrating the initial location (A) and the patterns of growth (B). SSC indicates semicircular canal; sv, scala vestibuli.
- Fig 6.
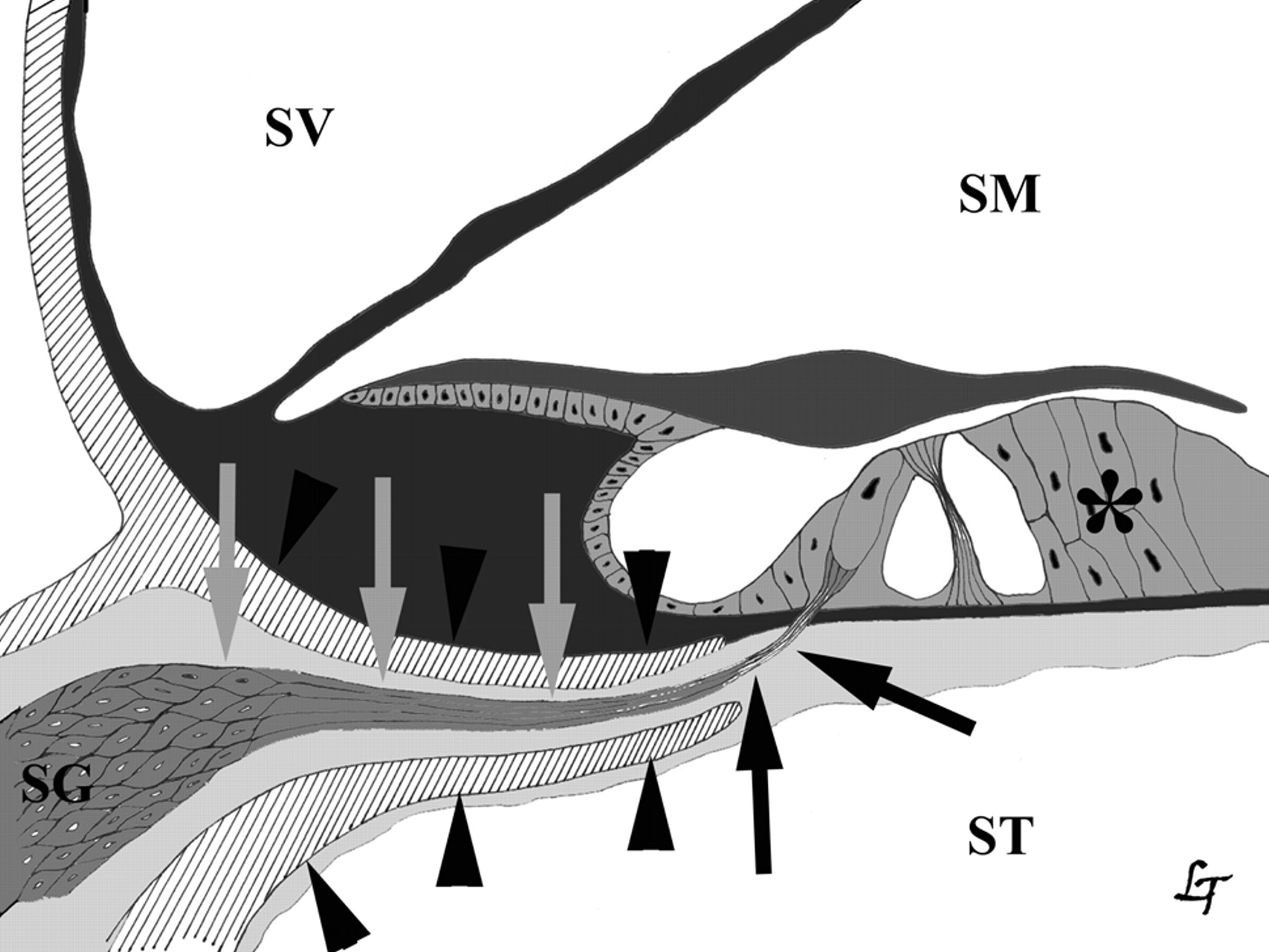
Anatomic relationship between cochlear nerve and scala tympani (ST). Cochlear nerve (gray and black arrows), organ of Corti (*), osseous spiral lamina (black arrowheads). SG indicates spiral ganglion; SM, endolymph in scala media; SV, perilymph in scala vestibuli.
- Fig 7.
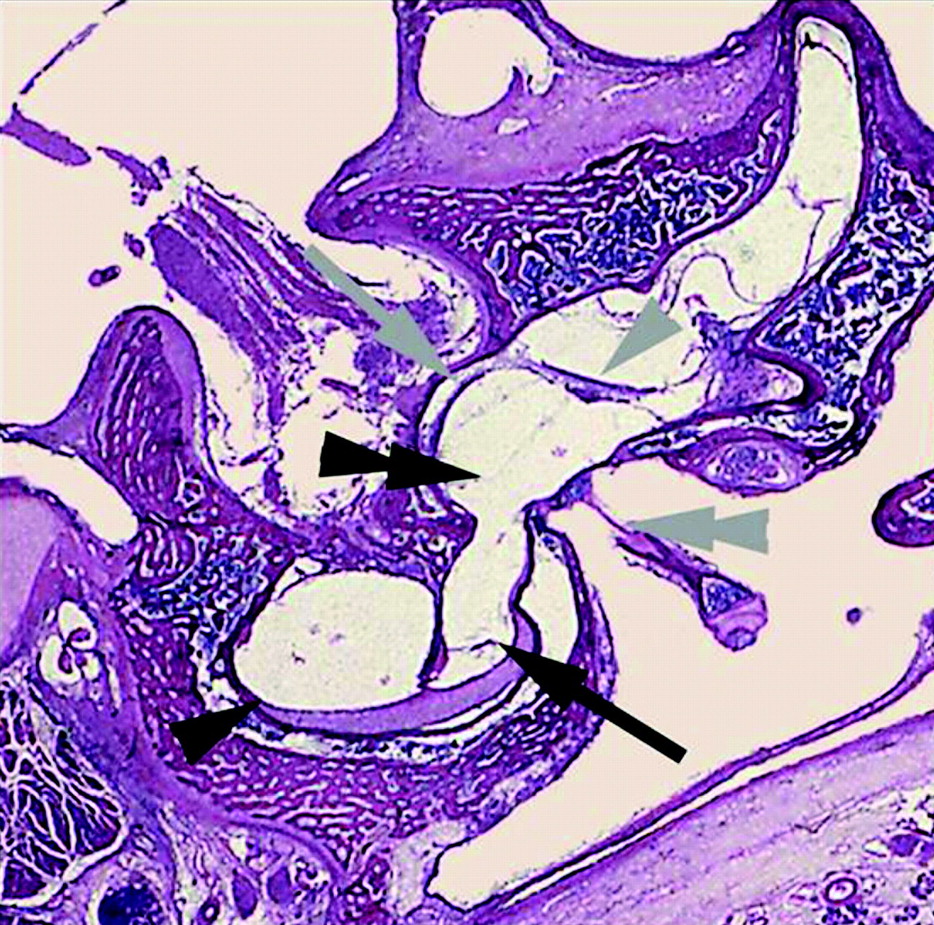
Coronal histologic section through the transition area of the basal turn of the left cochlea and the anteroinferior part of the left vestibule. Perilymph inside scala vestibuli (black arrow) is continuous with perilymphatic space around the saccule (double black arrowhead). No connection between the perilymph inside the scala tympani (black arrowhead) and perilymph inside vestibule. Macule of the saccule (gray arrow) and utricle (gray arrowhead), stapes with footplate inside the oval window (double gray arrowhead). Permission to publish obtained from Prof Dr F. Veillon and Prof Dr H. Sick, CHU Strasbourg, Hôpital Hautepierre, France.
- Fig 8.
Drawing of the intralabyrinthine perilymph (light gray) and endolymph (dark gray) spaces with indication of ILS extension routes. Intracochlear growth from scala tympani (ST) to scala vestibuli (SV; black arrowheads). ST ends at round window (white arrowheads). Growth from cochlea into vestibule and vice versa through the anatomic open connection between perilymphe in ST and perilymphatic space around the saccule (black arrows). ME indicates middle ear cavity; S, endolymph in saccule, stapes (double black arrowhead); U, endolymph in utricle.








Tables
Equipment Coil Type Field Strength, T Gd-Enhanced T1-Weighted Sequence T2-Weighted Sequence Sequence Type Section Thickness, mm In-Plane Resolution, mm × mm Sequence Type Section Thickness, mm In-Plane Resolution, mm × mm Siemens Magnetom Birdcage head 1 SE 3 0.80 × 0.80 3D CISS 0.7 0.65 × 0.65 Siemens Magnetom Vision Birdcage head 1.5 SE 2 0.90 × 0.90 3D CISS 0.7 0.37 × 0.37 Siemens Avanto Surface coils 1.5 MPRAGE 1 0.45 × 0.45 3D-TSE 0.5 0.53 × 0.53 GE Signa Surface coils 1.5 FSE 2 0.35 × 0.35 3D-FSE 0.8 0.39 × 0.39 Philips Intera Surface coils 1.5 3D-FFE 1.2 every 0.6 0.70 × 0.70 DRIVE25,26 0.7 every 0.35 0.36 × 0.36 Philips Achieva Surface coils 3 3D-FFE 1.2 every 0.6 0.60 × 0.60 DRIVE 0.6 every 0.3 0.43 × 0.43 Note:—SE indicates spin-echo; MPRAGE, magnetization-prepared rapid acquisition of gradient echo; FFE, fast-field echo; CISS, constructive interference in steady state; TSE, turbo spin-echo; FSE, fast spin-echo; DRIVE, driven equilibrium; Gd, gadolinium.
- Table 2:
Intralabyrinthine distribution of the 52 intralabyrinthine schwannomas at initial MR imaging
Initial Lesion Location No. of Patients, % Intracochlear 42 (80.7) Basal turn 4 (7.7) ST 3 (5.8) SV + ST 1 (1.9) Second turn 10 (19.2) ST 9 (17.3) SV + ST 1 (1.9) Apical turn 6 (11.5) ST 4 (7.7) SV + ST 2 (3.8) Basal turn + second turn 17 (32.7) ST 8 (15.4) ST and SV of both turns 5 (9.8) ST basal turn and ST + SV second turn 3 (5.8) ST + SV basal turn and ST second turn 1 (1.9) Apical turn + second turn 5 (9.5) ST 2 (3.8) SV 1 (1.9) ST apical turn and SV + ST second turn 2 (3.8) Intravestibular 7 (13.5) Anterior portion 1 (1.9) SCCs 2 (3.8) (Anterior + posterior) vestibule + SSC 3 (5.8) Anterior vestibule + SCCs 1 (1.9) Anterior vestibula + all cochlear turns 3 (5.8) Note:—ST indicates scala tympani; SV, scala vestibuli; SCC, semicircular canal.
No. Initial MR imaging Follow-Up Exam(s) Cochlear Labyrinth Vestibular Labyrinth Cochlear Labyrinth Vestibular Labyrinth IAC Apical Turn Second Turn Basal Turn Vestibule SCC Apical Turn Second Turn Basal Turn Vestibule SCC 1 ST ST + SV 2 ST ST + SV 3 ST + SV ST ST + SV ST + SV 4 ST ST + SV ST + SV ST + SV ST + SV Y 5 ST ST ST + SV 6 ST ST ST 7 ST ST ST + SV ST 8 ST ST ST + SV ST + SV Y 9 ST + SV ST + SV ST + SV ST + SV Ant + pos Y 10 ST + SV ST + SV ST + SV ST + SV Ant 11 ST + SV ST + SV ST + SV Ant ST + SV ST + SV ST + SV Ant + pos Lsc 12 ST + SV ST + SV ST + SV Ant ST + SV ST + SV ST + SV Ant 13 Ant Lsc SV Ant + pos Lsc + ssc + psc 14 Ant + pos Lsc + ssc Ant + pos Lsc + ssc + psc 15 ST + SV ST + SV ST + SV ST + SV 16 Ant SV Ant + pos Lsc Note:—ST indicates scala tympani; SV, scala vestibuli; Ant, anterior; pos, posterior; Lsc, lateral semicircular canal; ssc, superior semicircular canal; psc, posterior semicircular canal; IAC, internal auditory canal; Y, yes; SCC, semicircular canal.
Variable No. of Patients (%) Indication Tumor growth 4 (33.0) Prevention 6 (50.0) Vertigo 1 (8.3) Intrameatal extension 1 (8.3) Surgical approach Transmeatal 4 (33.0) RA, TC 5 (42.0) RA, TL 2 (17.0) RA, TO 1 (0.8) Benign schwannoma on pathological examination 12 (100.0) Note:—RA indicates retroauricular; TC, transcanal; TL, translabyrinthine; TO, transotic.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}