
Abstract
SUMMARY: Although the combination of MR imaging findings and clinical evidence of hypertension may suggest the diagnosis of posterior reversible encephalopathy syndrome (PRES), MR imaging findings with only involvement of the medulla oblongata pose a diagnostic dilemma. In the cases presented here, we demonstrated MR imaging findings of a presumed brain stem (medulla oblongata) variant of PRES and emphasized the diagnostic value of diffusion-weighted imaging (DWI).
Posterior reversible encephalopathy syndrome (PRES) is characterized by headache, vomiting, altered consciousness, seizure, and cortical blindness associated with imaging findings of predominantly posterior bilateral symmetric subcortical and cortical edema without frank infarction.1 Hyperintense lesions on T2-weighted MR imaging and swelling of the brain stem may be related to many different pathologic processes. PRES rarely presents with predominant involvement of the brain stem, and involvement of only the medulla oblongata is uncommon.2,3 Only 1 patient with PRES was reported to have medulla oblongata, upper cervical spinal cord, and supratentorial involvement.4 Herein we report 2 cases of a presumed variant of PRES with only medulla oblongata involvement.
Case Reports
Case 1
A 59-year-old man with history of left putaminal hemorrhage 15 years previously had a 1-week history of poor appetite, vomiting, altered consciousness, and seizure-like movements. His history was also significant for hypertension controlled with medications. Initial blood pressure (BP) was 210/108 mm Hg. Serum electrolytes were normal. Brain MR imaging (Signa LX2; GE Healthcare, Milwaukee, Wis) revealed isointensity on T1-weighted images (T1WIs) and diffusion-weighted images (DWIs), and hyperintensity on T2-weighted images (T2WIs) of the medulla oblongata and upper cervical spinal cord (Fig 1). Because of clinical signs and history and MR imaging findings of edema (not infarction) in the medulla oblongata and upper cervical spinal cord, the differential diagnosis included a variant of PRES, encephalitis, and encephalomyelitis. Because there was no evidence of infection or fever, and results on CSF examination were unremarkable, a variant of PRES was the likely diagnosis. An angiotensin-converting enzyme inhibitor and a calcium channel blocker were administered for BP control. His clinical condition improved, BP normalized to 140/90 mm Hg, and level of consciousness returned to normal. MR imaging 45 days later (Fig 1) indicated resolution of hyperintensity confirming a variant of PRES secondary to hypertension with involvement of the medulla oblongata.

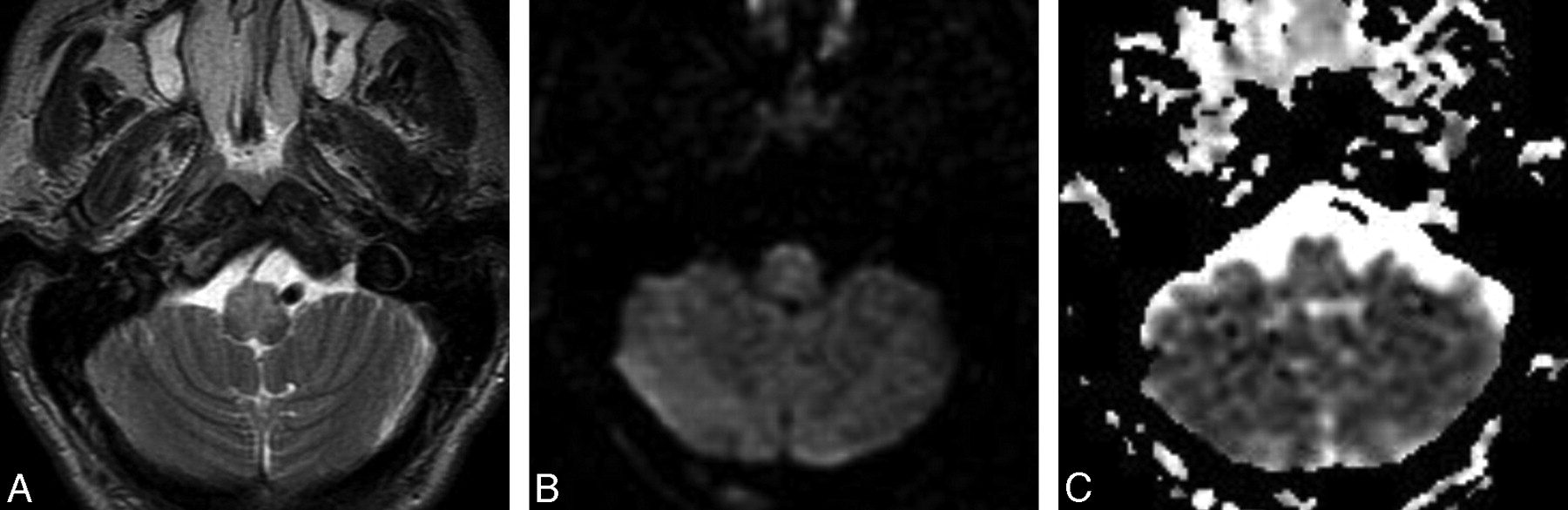
Case 1. A 59-year-old man with altered consciousness and elevated BP. A, MR imaging showing hyperintensity on T2W1 image of the medulla oblongata and upper cervical cord. B, Diffusion-weighted imaging shows normal intensity in the medulla oblongata. C, After BP control, hyperintensity on T2W1 image is resolved.
Case 2
A 62-year-old man with a history of hypertension and cerebral infarction was seen with a 3-day history of headache, vomiting, involuntary movement, and change in consciousness. BP was 180/100 mm Hg. No signs of infection or a meningeal abnormality were present, and serum electrolyte levels and CSF were normal. Brain MR imaging showed hyperintensity on T2WIs and isointensity on DWIs, which involved the medulla oblongata (Fig 2). No enhancement was noted after intravenous contrast administration. On the basis of clinical signs and history and MR imaging findings of vasogenic edema (not infarction or tumor) in the medulla oblongata, the most likely diagnosis was a variant of PRES. An angiotensin-converting enzyme inhibitor and a calcium channel blocker were administered, and BP normalized to 140/80 mm Hg. His clinical condition returned to baseline 5 days later, and no neurologic deficit was noted, confirming the diagnosis of a variant of PRES with involvement of the medulla oblongata. The patient refused follow-up MR imaging; however, he remains alive and well at follow-up in the neurology department.

Case 2. A 62-year-old man with headache, altered consciousness, and elevated BP. MR imaging showing hyperintensity on T2W1 image and normal signal intensity on DWI/ADC map involving the medulla oblongata; A, MR imaging showing hyperintensity on T2WI image involving the medulla oblongata; B, Diffusion-weighted imaging showing normal signal intensity in the medulla oblongata; C, ADC map showing normal signal intensity in the medulla oblongata.
Discussion
PRES typically involves the parieto-occipital lobes; the subcortical white matter and cortex of the posterior circulation are most commonly involved. Involvement of the basal ganglia and brain stem is much less frequent. Atypical PRES predominantly involves regions other than the parieto-occipital lobes. In these patients, high signal intensities on T2WIs are noted in the frontal lobe, basal ganglia, thalamus, brain stem, and subcortical white matter.3,5 The brain stem may be involved in combination with other regions of the brain (supratentorial PRES). In a report by Weingarten et al,6 15 of 36 patients with acute hypertensive encephalopathy had T2-hyperintense brain stem lesions of varying sizes; however, cases predominantly affecting the brain stem were rare. Brain stem variants of PRES should be differentiated from brain stem infarction, pontine glioma, central pontine myelinolysis, and infective encephalitis because the neurologic symptoms are reversible with prompt treatment.
PRES arises from failure of cerebrovascular autoregulation at high BPs, which results in cerebral hyperperfusion, disruption of the blood-brain barrier, and vasogenic edema.7 Autoregulation maintains a constant blood flow to the brain despite systemic BP alterations through arteriolar constriction and dilation.7 In animal models, there is an upper limit of BP at which cerebral autoregulation fails. At this breakthrough point, constricted arterioles dilate because of increased BP, and the increased perfusion overcomes the blood-brain barrier, allowing extravasation of fluid, macromolecules, and red blood cells into brain parenchyma.8 Pathologic examinations of brains with PRES reveal interstitial edema, petechial microhemorrhages, and fibrinoid necrosis within the arteriole walls, and little or no evidence of infarction.9
Abnormal autoregulation as the pathophysiologic process responsible for PRES is supported by MR imaging DWI and apparent diffusion coefficient (ADC) alterations. Studies suggest that lesions of hypertensive encephalopathy and PRES represent vasogenic rather than cytotoxic edema in most cases.10 In cases of PRES, areas of increased signal intensities on T2WIs show increased ADC values, representing vasogenic edema.10 This may be useful in differentiating PRES from infarction and other metabolic brain disorders with cytotoxic edema in which ADC mapping values are decreased and signal intensities are higher than those of surrounding brain tissue on DWI.11 Furthermore, studies using diffusion tensor imaging revealed that the anisotropy index of PRES patients decreases in proportion to the increase in water diffusion characteristics confined largely to cortical gray matter and subcortical white matter, which supports vasogenic edema from cerebrovascular autoregulatory dysfunction is the pathophysiologic mechanism of uncomplicated PRES.12
Studies have shown that sympathetic innervation of cerebral circulation confers a protective effect from increases in systemic BP.7 Because the anterior cerebral circulation (internal carotid system) has greater sympathetic innervation than the posterior circulation (vertebrobasilar system), the systemic BP increases breakthrough vasodilation, and vasogenic edema occurs first in a vertebrobasilar vascular distribution. Thus, lesions occur first in the occipital lobes, cerebellum, brain stem, and medulla oblongata.
The cases presented illustrate MR imaging findings of a variant of PRES with only involvement of the medulla oblongata and emphasize the diagnostic value of DWI. By familiarizing radiologists with these entities, it is hoped that atypical cases of PRES will be recognized earlier and appropriate management instituted in a timely fashion.
References
- Received July 21, 2008.
- Accepted after revision August 27, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}