
Abstract
BACKGROUND AND PURPOSE: In recent years, effort has been made to study 3D biometry as a method for fetal brain assessment. In this study, we aimed to compare brain volumes of fetuses with cytomegalovirus infection and noninfected controls. Also, we wanted to assess whether there is a correlation to their neurodevelopmental outcome as observed after several years.
MATERIALS AND METHODS: A retrospective cohort study examined MR imaging brain scans of 42 fetuses (at 30–34 weeks' gestational age) that were diagnosed with intrauterine cytomegalovirus infection. Volumetric measurements of 6 structures were assessed using a semiautomated designated program and were compared with a control group of 50 fetuses. Data collected included prenatal history and MR imaging and sonographic and neurodevelopmental follow-up.
RESULTS: We found that all brain volumes measured were smaller in the cytomegalovirus-infected group and that there was a correlation between smaller cerebellar volume and lower Vineland II Adaptive Behavior Scales questionnaire scores, especially in the fields of daily living and communication skills.
CONCLUSIONS: In this study, we found that brain volumes are affected by intrauterine cytomegalovirus infection and that it has a developmental prognostic meaning. Such information, which should be supported by further research, may help clinicians further analyze imaging data to treat and make a better assessment of these fetuses.
ABBREVIATIONS:
- CMV
- cytomegalovirus
- CV
- cerebellum volume
- ICC
- intraclass correlation coefficient
- LEBV
- left eyeball volume
- LHV
- left hemisphere volume
- REBV
- right eyeball volume
- RHV
- right hemisphere volume
- STV
- supratentorial volume
- VABS-II
- Vineland II Adaptive Behavior Scale
Cytomegalovirus (CMV) infection is the most common intrauterine infection, affecting 0.3%–2% of live-born neonates.1 Only 10%–20% of infected fetuses will show signs of infection at birth: intrauterine growth restriction, microcephaly, hepatosplenomegaly, thrombocytopenia, brain parenchymal calcifications, ventricle enlargement, cerebellar hypoplasia, and so forth. Different neurodevelopmental sequelae such as mental retardation and motor/hearing or visual impairment can manifest later in life, even in asymptomatic neonates.2
Because CMV is the most common environmental cause of sensorineural hearing loss and a relatively common cause of mental retardation,3 it is important to improve the clinicians' ability to assess and predict the outcome of congenital CMV infection in order to provide the most accurate counseling to worried couples.
Today, the main assessment modalities of CMV-infected fetuses are sonography and 2D MR imaging.4 In recent years, the possibility of using 3D biometrics as a tool for fetal brain assessment has been investigated.5⇓⇓–8 This area is innovative with very limited information in the literature. There were only a few studies on quantitative MR imaging in CMV,9 but none had a follow-up or tried to examine a correlation to future outcomes. This type of quantitative information can lead to a better understanding of CMV infection effects on the developing brain, especially if correlated with the neurodevelopmental outcome.
In this study, we aimed to compare volumetric measurements of different structures in the fetal brain between CMV-infected fetuses and a control group of noninfected fetuses. In addition, we wanted to examine the correlation between brain volumes of the infected fetuses and their developmental outcome as observed after several years.
Materials and Methods
Subjects and Settings
This is a historic prospective cohort study that examined all cases (between January 2009 and June 2014) of women with CMV infection during pregnancy who underwent fetal MR imaging in our Chaim Sheba medical center (all CMV-infected women are indicated for clinical, MR imaging, and sonographic follow-up).
Forty-two fetuses were recruited according to the following criteria:
1 MR imaging was performed due to maternal primary CMV infection.
2 CMV infection occurred periconceptionally or during the first or second trimester of pregnancy.
3 Amniocentesis was performed and confirmed fetal CMV infection.
4 Fetal brain MR imaging was performed at 30–34 weeks' gestational age.
5 The developmental outcome was checkable (women who underwent termination of pregnancy were not included).
6 The data regarding pregnancy, follow-up, delivery, and outcome were available (women with a lack of information or who refused to answer the Vineland questionnaire were not included).
7 The MR imaging scans were of fair quality, enabling us to perform the necessary measurements.
The measurements were compared with those of a control group composed of 50 fetuses that underwent MR imaging for a non-neurologic reason as a part of a different cohort study performed in our institution, using the same semiautomated program.10 These scans were obtained at the same gestational ages and were found to contain no brain pathology according to a neuroradiologist's expert opinion. The scans Source, the measuring methods, and the volume calculations were identical.
To assess volume differences between the cases in the study and the control group that were measured in different gestational weeks, we created a z score for each brain volume of the case group using the means and SDs of each gestational week of the control group.
Data obtained from medical records included the following: pregnancy history, infection history, sonographic and MR imaging follow-up findings, perinatal history, and medical follow-up.
MR Imaging and the Semiautomated Algorithm
Fetal brain MR imaging was performed using a 1.5T system (Optima MR450w, 70 cm bore scanner; GE Healthcare, Milwaukee, Wisconsin). Single-shot fast spin-echo T2-weighted sequences in 3 orthogonal planes were performed using the half-Fourier technique (NEX = 0.53) with the following parameters: section thickness = 3 or 4 mm, no gap, flexible coil (8-channel cardiac coil), FOV determined by the size of the fetal head with a range of 24 × 24 cm to 30 × 30 cm, acquisition time between 40 and 45 seconds, matrix = 320 × 224, TE = 90 ms, TR = 1298 ms, pixel bandwidth = 122 Hz/pixel, specific absorption rate values = 1.1–1.7 W/kg.8
The algorithm is a recent development of our group.10 It is based on an initial contour manually drawn in the brain parenchyma of the midcoronal slice that defines the origin of interest. The initial contour is then automatically propagated by a level-set-based active contour algorithm until convergence into a new contour. The convergence is based on the representative pixels that are included in the initial contour. The next step is forward and backward propagation starting at the midcoronal slice, achieving contours automatically for every slice. Each new contour is based on the previous one, with a prefixed downsize volume for every slice. When it is completed, the user can adjust the resulting contour to achieve maximal accuracy. The volume is computed as the total number of voxels enclosed by the contours multiplied by the voxel size.
Measurements
All measurements were obtained in the coronal plane. For each fetus, we measured 8 structures: the supratentorial brain, right and left cerebral hemispheres, right and left lateral ventricles, right and left eyeballs, and the cerebellum. Measurements were used as follows (Fig 1). Of the volumes measured, 6 structures were assessed in the study:

Representative slices of structure boundaries; A, STV and CV. B, REBV and LEBV.
Supratentorial Brain.
We included the parenchyma of the frontal, parietal, occipital, and temporal lobes (including the third ventricle) and excluded the lateral ventricles (measured separately and subtracted), the brain stem, the cerebellum, and the fourth ventricle. Anterior, posterior, superior, and lateral boundaries were defined as the outer edge of the cerebral cortex. The inferior border matched the cortex and an imaginary line crossing the brain stem between the edges of the tentorium cerebelli.
Hemispheres (Right Hemisphere Volume [RHV] and Left Hemisphere Volume [LHV]).
The volumes were measured separately using the same lateral boundaries, with the Sylvian fissure as a medial boundary and excluding the lateral ventricles.
Cerebellum.
We included the cerebellar peduncles and vermis. The brain stem and the fourth ventricle were excluded.
Eyeballs (Right Eyeball Volume [REBV] and Left Eyeball Volume [LEBV]).
Eyeballs were defined as the vitreous body and the lens, excluding the optic nerve.
The intraclass correlation coefficient (ICC) and limits of agreement were used to study the reliability of the measurements across measurers. Interobserver variability was tested comparing measurements of 15 fetuses made by 2 independent observers. Intraobserver variability was tested by repeating measures of 15 fetus samples. Results were defined as poor for ICC < 0.6, satisfactory agreement for 0.6 < ICC < 0.8, good for 0.8 < ICC < 0.9, and excellent for ICC > 0.9.
Neurodevelopmental Outcome
Children were evaluated using the Vineland II Adaptive Behavior Scale (VABS-II) questionnaire,11 which examines 4 areas of development from birth through adulthood:
1 Communication (receptive, expressive, written)
2 Daily living skills (personal, domestic, community)
3 Socialization (interpersonal relationships, play, leisure time, and coping skills)
4 Motor skills (gross, fine).
Because it is a norm-based instrument, the examinee's adaptive functioning is compared with that of others his or her age.
The standard score derived from this instrument has a mean of 100 ± 15, and the adaptive level is derived from it. Scores of children were considered abnormal if the standard score was <86 (below an adequate adaptive level).
The published Israeli version of the VABS-II questionnaire was administered, but no Israeli norms are available for the full age range. Because there was no reason to believe that children in Israel and the United States would develop mental and motor skills differently, we used the norms of the United States.12
Statistics
Categoric variables were expressed as number and percentages. Distribution of continuous variables was assessed using a histogram and Q-Q plot. Continuous variables were described using median and interquartile range or mean and SD as appropriate. The intraclass correlation coefficient was used to evaluate the inter- and intraobserver agreement.
Continuous variables were compared between the CMV-infected group and noninfected controls and also among individuals in the CMV-infected group, using an independent-samples t test or Mann-Whitney U test. The 1-sample Wilcoxon signed rank test was used to compare the calculated z scores of the CMV cohort to zero. The Spearman Correlation coefficient was used to evaluate the association among continuous variables.
A 2-tailed P < .05 was considered statistically significant. The false discovery rate method of Benjamini–Hochberg was used to conduct correction for multiple comparisons. Analyses were performed with SPSS Statistics for Windows (Version 24.0, 2016; IBM, Armonk, New York).
Ethics Approval
The study was approved by the Sheba Medical Center institutional review board (No. 0256-13-SMC).
Results
Population
A total of 95 singleton pregnant women diagnosed with periconceptional and first- and second-trimester CMV infection were assessed in our clinic during the study period (between January 2009 and June 2014). Of these women, 36 did not undergo MR imaging in our institution, 2 underwent termination of pregnancy, and 4 fetuses tested negative for CMV infection with amniocentesis. Six other women were excluded because MR imaging was performed in a gestational week not matching our criteria. Five more women were excluded for poor-quality MR imaging scans. Overall, 42 fetuses were eligible according to the study criteria.
Clinical Characteristics
From the main population of CMV-infected pregnant women, 2 (4.8%) women were infected around conception; 20 (47.6%), during first trimester; and 20 (47.6%), during the second trimester. Imaging follow-up during pregnancy found 15 women (35.7%) with abnormal findings on fetal sonography and 9 women (21.4%) with abnormal findings on fetal brain MR imaging. More clinical characteristics of pregnancies and fetuses of our study are described in On-line Table 1.
Delivery and outcome characteristics are described in On-line Table 2. Fourteen fetuses (33.3%) had abnormal perinatal outcomes, and 13 (31%) had abnormal findings on brain sonography at birth. Of those neonates, 18 (42.8%) were treated with ganciclovir, with a median time of 12 months (interquartile range, 12–12 months). Clinical retrospective follow-up of these children revealed that 2 (4.8%) had motor impairment, 6 (14.3%) had auditory impairment, and 4 (9.5%) had auditory impairment that resolved after treatment with ganciclovir.
Intra- and Interobserver Variability Assessment
The results of inter and intraobserver reliability of measurements are shown in On-line Table 3.
The volume measurements of the supratentorial volume (STV), right hemisphere volume, left hemisphere volume, cerebellum volume (CV), and Left Lateral Ventricle Volume (LLVV) showed excellent intra- and interobserver reliability: The lowest ICC for volume was 0.94. ICC measurements of right eyeball volume and Right Lateral Ventricle Volume (RLVV) showed good interobserver reliability, and left eyeball volume showed satisfactory interobserver reliability.
Volumetric MRI Results
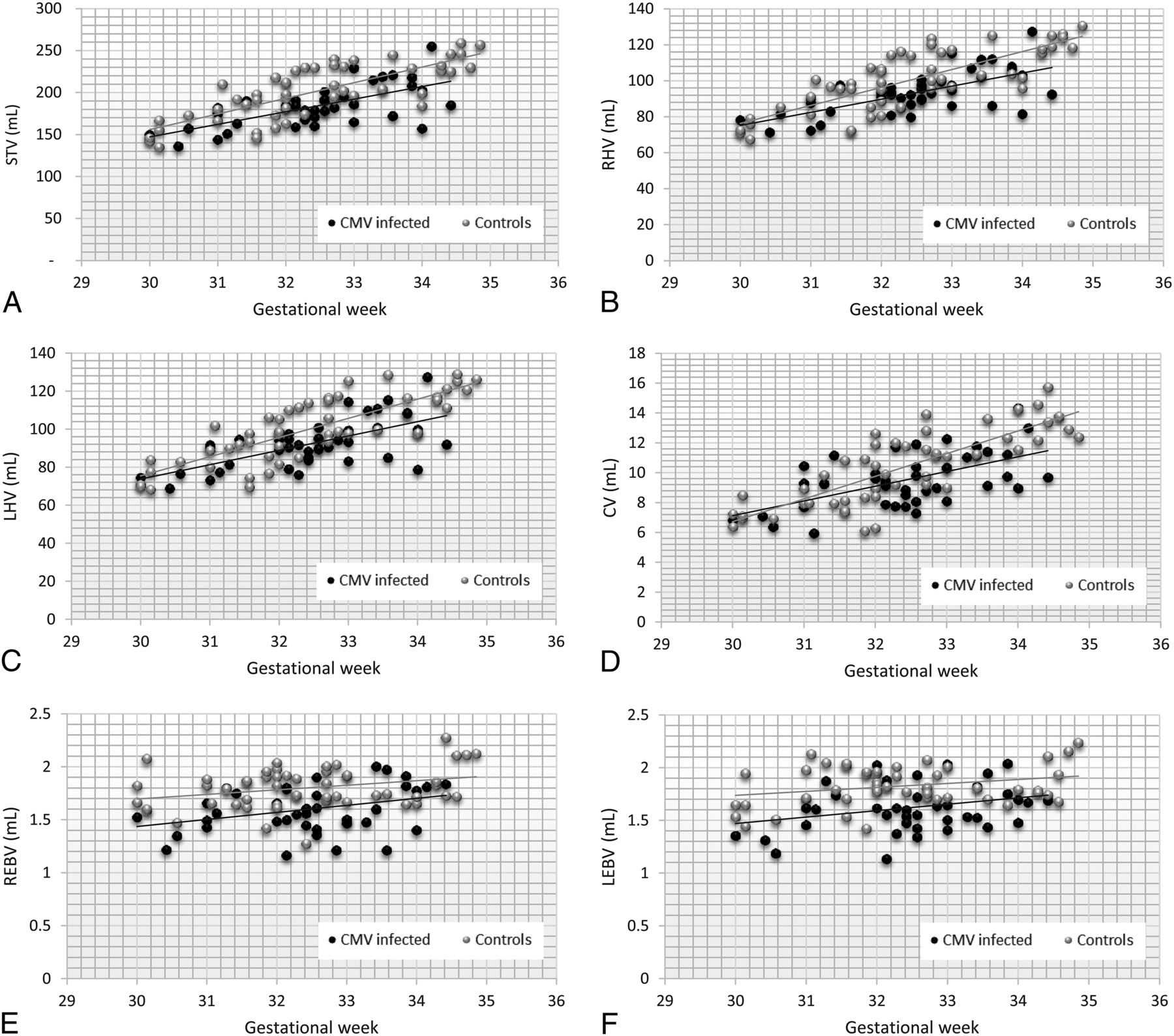
Scatterplots of volumetric measurements according to gestational age of the CMV-infected group and the noninfected controls are presented in Fig 2. Table 1 presents the means or medians of the volumes found in the case group (fetuses with CMV infection) compared with the control group (noninfected fetuses). As shown, each volume of brain structures we examined was smaller in the case group; the cerebellum was the only structure that was smaller, but with a statistically insignificant difference. To overcome the volume differences resulting from measurement in different gestational weeks, we standardized the volumes of the CMV-infected group to the z score using the means of the volumes of the control group (healthy population) for each gestational week during MR imaging, as presented in Table 2. We showed, for all brain volumes measured, that z is always below zero, with a significance level of <.05; hence, we proved that when neutralizing gestational age as a confounder, all volumes (STV, RHV, LHV, CV, REBV, LEBV) of the case group (CMV-infected fetuses) are smaller and, specifically, <1 SD from the volumes of the controls (P ≤ .001).

Scatterplots of volumetric measurements according to the gestational age of the CMV-infected group and the noninfected controls. Simple linear regression lines are shown for each set of data. A, STV. B, RHV. C, LHV. D, CV. E, REBV. F, LEBV.
Means/medians of brain volume measurements for CMV-infected and control groupsa
Brain volumes of CMV-infected fetuses demonstrated as z scoresa
Neurologic and Developmental Outcome
Neurologic and developmental outcome was assessed using the Vineland II Adaptive Behavior Scales (characteristics of the Vineland adaptive level results are described in On-line Table 4). The mean age of children evaluated was 3.4 years (range, 2.2–4.2 years). Two children (4.8%) had moderately low communication skills, 3 (7.1%) had moderately low daily living skills scores, 5 (11.9%) had moderately low social skills scores, 4 (9.5%) had moderately low motor skills scores, and 3 (7.1%) had moderately low complete adaptive behavior results. Abnormal outcome was established on the basis of the following: 1) VABS-II results of any category were below adequate, 2) motor impairment was seen in clinical follow-up, or 3) there was any hearing impairment (present or treated with ganciclovir). From our study population, 14 children were defined by the criteria mentioned above as having abnormal neurologic and/or developmental outcomes (see their characteristics in On-line Table 5).
Volumetric Measurements and Neurodevelopmental Outcome
We used the Spearman rank correlation coefficient test to examine the correlation between brain volumes (represented by z scores) and the developmental outcome (represented by the Vineland II standard scores). We found a correlation between cerebellar volume and daily living skills: The smaller the cerebellum volumes were, the bigger the impairment in daily living skills was, with a significance of .041. When corrected for multiple comparisons, this correlation became insignificant (P = .246). We have not found any other significant correlation to VABS-II results (On-line Table 6).
Then we compared the VABS-II results obtained in very small brain volumes (<2 SDs of the z score) with the VABS-II results of all the rest (above −2 SDs of the z score). We found that a small fetal cerebellum was associated with a lower Vineland score of the child in the fields of communication (significance of .027), daily living skills (significance of .009), and overall adaptive level (significance of .043). After we corrected for multiple comparisons, only the association between a small fetal cerebellum and daily living skills stayed significant (P = .045). We have not found a significant correlation to motor skills or social skills, or with any other brain volume we measured (On-line Tables 7 and 8).
We have not found a significant correlation between brain volumes and any other clinical outcome in our study group such as hearing impairment (present or past) or findings on brain sonography at birth (small for gestational age). We have also not found a correlation between brain volumes and trimester of infection (On-line Table 9).
Discussion
In this study, we compared brain volumes of fetuses with intrauterine CMV infection and noninfected controls. We also assessed their neurologic and developmental outcome as observed after several years. We found that all brain volumes measured were smaller in the CMV-infected group and that there is a correlation between cerebellar volume and developmental outcome.
Our study joins the growing amount of research in the new field of quantitative MR imaging. A 3D assessment provides information on the volume of different brain structures; thus, much can be learned and deduced about normal brain development and brain pathologies.7,13,14 A few studies have already shown some interesting results using quantitative MR imaging in the research of heart disease, idiopathic ventriculomegaly, and intrauterine growth restriction.5,6,8 There were only a few studies on quantitative MR imaging in CMV-infected fetuses, but none included a follow-up or tried to examine a correlation to future outcomes. Hoffmann et al9 examined the volume of hemispheres and temporal lobes in 27 fetuses with intrauterine CMV infection, and compared with a control group of healthy fetuses, temporal lobe volumes, normalized to whole, were smaller than the volumes in the noninfected control group. Our study contributes to and renews the knowledge of quantitative MR imaging in CMV-infected fetuses and demonstrates a statistically significant decrease (of >1 SD) in the supratentorial, both hemispheric, eyeball, and cerebellum volumes.
We assume that the fetal brain volume decrease is attributed to the brain damage caused by the viral infection. The damage is a combined result of some possible mechanisms: loss of neural stem cells and intermediate progenitors; interruption to stem cell migration and cell differentiation processes; astroglia insult, and therefore disruption of their supportive functions in the brain; neurotoxicity due to the inflammatory processes; and hypoxia due to severe placentitis.15
In this study, we also found a correlation between lower cerebellar volumes and lower VABS-II scores, specifically in the fields of communication and daily living skills. The cerebellum is considered particularly vulnerable to the negative effect of an insult due to its rapid growth during gestation.16 There is an association between cerebellar injury and neurodevelopmental sequelae, including cognitive, language, behavioral, social, and motor deficits.17 Children with congenital CMV infection exhibit a range of disabilities in these areas2; therefore, the findings of the effect on the cerebellar volume may be of great importance during follow-up and postinfection counseling.
The time of infection has a prognostic significance; most fetal and neonatal sequelae are associated with first- or second-trimester infections.18,19 Because the risk of an abnormal outcome of the fetus with third-trimester infection is minimal, we focused on patients who acquired primary CMV infection during the first and second trimesters. Hoffmann et al9 found, in their research, that infection during the first and second trimesters had a greater effect on volume differences than in the third trimester. In our research, we did not find a connection between the trimester of infection and brain volumes; perhaps a larger sample size is needed. Also, in this study, we did not find a correlation between brain volumes and hearing impairment; this may be due to several reasons: a small sample size or the pathogenesis of the sensorineural hearing loss possibly being different from the pathogenesis that causes decreased brain volumes.
The importance of this study is not only in its results, but we also demonstrate the use of a new tool, a semiautomated designated program that enables easy measurement of brain volumes that is less time-consuming and user-dependent. By applying this method in pathologic and healthy brain research, we believe that fetal brain volumetry can turn from a research tool into a practical clinical one.
We acknowledge some limitations of this study. First, we decided not to include pregnancies that underwent termination because one of our main goals was to find correlation to the outcome. However, there might be an importance in characterizing these fetuses because it might be reasonable to think that they might have had more severe findings. Also, we had a small sample size due to difficulty in finding women who met all the inclusion criteria. Nevertheless, this study was able to produce statistically significant statements and is relatively not small compared with other fetal volumetric studies.8,9 Also, the control group from which the normal volumes were derived was not composed of fetuses of volunteers but belonged to a cohort of patients with either a suspected brain pathology dismissed by MR imaging or a family-related history. Lack of healthy pregnant women for reference is a common limitation in this research field.13,20
Conclusions
Our study shows that in first- and second-trimester primary CMV intrauterine infection, brain volumes are affected, what bears a developmental prognostic meaning. There is a need to continue to explore this field of quantitative MR imaging and its ability to predict abnormal outcome in CMV-infected fetuses, with larger sample sizes and multi-institutional studies, to obtain significant results to characterize these volume differences, provide a deeper insight of the neurologic and developmental outcome, and influence important decision-making.
Footnotes
Anya Grinberg and Eldad Katorza contributed equally to this work.
References
- Received September 3, 2018.
- Accepted after revision December 1, 2018.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}