
Abstract
BACKGROUND AND PURPOSE: Intracranial pressure modifications caused by a skull defect, such as craniectomy or craniotomy, may change the hemodynamics and decrease the accuracy of CTA to confirm brain death. This study aimed to evaluate the impact of a skull defect and the interpretation criteria of images on this diagnostic test.
MATERIALS AND METHODS: A series of consecutive patients with a clinical diagnosis of brain death underwent CTA (case group), while the control group comprised patients with acute ischemic stroke in the same period. CTA criteria adopted to confirm brain death were the absence of opacification of the M4 branches and internal cerebral veins. The evaluation also included the presence of “stasis filling.” Cases were stratified as intact skull, craniotomy, and craniectomy. Three neuroradiologists evaluated all examinations independently.
RESULTS: In the case group, according to the Frampas criteria, the sensitivity of CTA to confirm brain death was 95.5% in patients with intact skull, 87.5% with craniotomy, and 60% with craniectomy. False-negative diagnoses of brain death were 15.6%, related to stasis filling in 71.4% (P < .001). However, according to the “modified Frampas criteria,” the sensitivity of CTA to confirm brain death was 100% in patients with intact skull, 93.8% with craniotomy, and 80% with craniectomy. False-negative diagnoses of brain death were found in 6.2% of patients, and there was no stasis filling. CTA showed 100% specificity in the control group. There were no disagreements among observers.
CONCLUSIONS: CTA had a high diagnostic accuracy and reproducibility to confirm brain death in patients with an intact skull. The modified Frampas criteria increased the sensitivity of CTA, particularly in patients with a skull defect. A concurrent skull defect, especially craniectomy, can decrease the sensitivity of CTA to confirm brain death.
ABBREVIATIONS:
- BD
- brain death
- ICM
- iodinated contrast medium
- ICV
- internal cerebral vein
- SD
- skull defect
- SF
- stasis filling
Brain death (BD) is the result of diffuse, progressive, and irreversible brain damage clinically characterized by a deep unresponsive coma and the absence of spontaneous ventilation and brain stem reflexes.1⇓–3 Although the clinical criteria for the diagnosis of brain death assess the absence of brain stem functions, some countries have used the concept of global brain death, adding ancillary tests to show the absence of brain circulation or absence of electric activity or absence of metabolic activity, including the cerebral hemispheres.4⇓–6 Circulatory evaluation is commonly used because it is subject to less pharmacologic interference (eg, the use of sedatives and occurrence of severe electrolyte and metabolic disorders).7,8
Conventional angiography is the criterion standard to evaluate the circulatory system.9⇓–11 However, because this method is invasive, is not widely available, and requires specialized neuroradiologic expertise to perform and interpret the results, other alternatives have been investigated, including CTA. The accuracy of CTA for a BD diagnosis was validated by Frampas et al12 through the absence of intracranial arterial opacification of the distal branches (M4) and internal cerebral vein (ICV), both evaluated in the venous series of CTA, showing moderate sensitivity (85.7%) and high specificity (100%). Other studies have confirmed similar accuracies.13⇓⇓⇓⇓–18 Nevertheless, the interpretation criteria of the images used by Frampas et al12 limited the applicability of CTA to confirm BD due to patients with false-negative findings (14.3%).
According to the Monro-Kellie doctrine, intracranial pressure is the result of the balance among the CSF, blood, and brain parenchyma inside the skull, a rigid compartment. Increased intracranial pressure results in pressure compensation through the displacement of the CSF to the spinal subarachnoid space, followed by intracranial vascular collapse. This collapse occurs initially in the venous compartment because of the increased compliance and lower intraluminal pressure and then in the arterial compartment, with consequent brain damage.19⇓–21
Therefore, a skull defect (SD) in patients with suspected BD, such as extensive fracture or operation (craniectomy or craniotomy), may decrease the intracranial pressure, changing the intracranial hemodynamics and decreasing the diagnostic accuracy of ancillary tests that evaluate brain circulation.10,22,23 However, there are no specific studies evaluating the accuracy of CTA for BD confirmation in patients with SD, to our knowledge.
Our aim was to evaluate the impact of SDs and the interpretation criteria of imaging on the accuracy of CTA for BD confirmation.
Materials and Methods
Study Design
This cross-sectional and observational study was conducted at a single hospital center (Santa Casa de Misericordia de São Paulo) between June 2012 and July 2014. A case series of consecutive patients with a clinical diagnosis of BD (reference standard determination of BD) was evaluated according to the legal requirement,24 the Brazilian BD protocol, which consists of 2 clinical examinations and some confirmatory ancillary tests, namely, transcranial Doppler (47 patients), conventional angiography (2 patients), and nuclear medicine (1 patient). In addition to the Brazilian BD protocol, these patients underwent CTA, the results of which did not interfere with the final diagnosis regarding BD. Due to the similarity between the stroke and BD protocols, the control group consisted of 22 patients with ischemic stroke who were candidates for thrombolysis and underwent CTA before any therapeutic proposal, in the same period. The institutional review board approved this study.
All patients older than 2 years of age with a BD clinical diagnosis, evaluated according to the legal requirements24 of the Brazilian BD protocol, were enrolled after their legal guardian and 2 witnesses agreed to participate in the study by signing the free and informed consent form. Patients were excluded when they had a mean arterial pressure lower than 80 mm Hg, if the guardians did not authorize study enrollment, if contraindications or the inability to receive intravenous iodinated contrast medium (ICM) was present, or if the technical quality of the images was deemed inadequate. Demographic and clinical data, including age, sex, cause of BD, and the time interval between the BD diagnosis and CTA, were collected in a data base.
Technical Data
All examinations were acquired in a 64–detector row CT scanner (Version v2.6.2.22004; Brilliance™ CT 64-channel scanner; Philips Healthcare, Best, the Netherlands) with a minimum dose of ionizing radiation25 following the CTA protocol proposed by Frampas et al.12
After lateral topography, 3 similar acquisitions were planned starting at the C1–C2 level to the cranial vertex. The first acquisition was an NCCT scan (120 kV; 350 mA). Iso-osmolar, nonionic intravenous ICM (iopromide, Ultravist 300; Bayer HealthCare, Berlin, Germany) was injected through the right antecubital vein at a rate of 4–6 mL/s using a dual-head power injector (Medrad Stellant® D, Bayer HealthCare, Indianola, Pennsylvania) and a 16- to 22-ga catheter, with a pressure limit of 325 psi, depending on the age range. The total volume administered throughout the protocol was calculated on the basis of the estimated weight of the patient (2.0 mL/kg, reaching a maximum of 50 mL). The second (arterial) and third (venous) acquisitions (120 kV, 185 mAs, 0.67-cm thickness, 0.33-cm increments, FOV of 450 mm, and automatic settings for pitch and release) were performed, starting 20 and 60 seconds after the ICM injection commenced.
Image Analysis
To evaluate hemodynamic repercussions resulting from the SD, we divided the patients into 2 different groups: the intact skull and SD groups. The patients with SDs were divided into 2 subgroups, those with craniotomy and craniectomy.
The NCCT series confirmed the adequate passage of intravascular ICM in all patients by identifying opacification of the superficial temporal arteries and upper orbital veins during the examination as well as differentiating between spontaneously hyperattenuating vascular content and delayed, weak, persistent, and progressive vascular opacification (pseudo-subarachnoid hemorrhage versus true vascular opacification).
The arterial and venous series enabled the assessment of vessel opacification in the intracranial arterial and venous compartments via CTA based on MIP postprocessing algorithms (thickness: 10 mm) in workstation (Extended Brilliance™ Workspace, Version 3.5.0.2250; Philips Healthcare).
The progressive opacification of the intracranial arterial compartment between early (arterial) and delayed (venous) acquisitions of CTA was analyzed. The delayed, weak, persistent, and progressive opacification of the intracranial arterial compartment found between early (arterial) and delayed (venous) acquisitions of CTA is known as “stasis filling” (SF). This phenomenon is commonly observed in angiographic studies.10,26,27
Three neuroradiologists with experience in the interpretation of CTA studies (9, 22, and 23 years, respectively) evaluated all the examinations independently using simultaneous viewing of images of the NCCT, arterial (early), and venous (delayed) CTA series. These findings were assessed to generate a single consensus report, which was compared with the BD clinical diagnosis (reference standard determination of BD).
Two sets of criteria were used to confirm BD by CTA. The original criteria proposed by Frampas et al,12 which consist of the absence of opacification of the M4 branches and ICV, both evaluated in the venous series of the CTA; and another set, called in this study the “modified Frampas criteria,” consisting of the absence of opacification of the M4 branches in the arterial phase and ICV in the venous phase of the CTA. The rationale for using these modified criteria is to avoid false-negative findings due to SF because opacification of the intracranial arterial compartment was evaluated in the arterial phase of CTA.
Statistical Analysis
Categoric variables were described by the absolute and relative frequencies and were compared using the χ2 test. The age and time interval between the clinical diagnosis of BD and CTA were assessed for normality using graphic methods and skewness and kurtosis values. Age was described using means and standard deviations and was compared using the Student t test for independent samples. The time interval was described using medians and quartiles and was compared using the Mann-Whitney test.
The accuracy of CTA in each group according to the presence and type of SD was determined using contingency tables and by calculating the sensitivity, specificity, and positive and negative predictive values. Interobserver agreement was evaluated using the Cohen κ, with the following interpretation: <0, no agreement; 0–0.19, very poor agreement; 0.20–0.39, poor; 0.40–0.59, moderate; 0.60–0.79, high; and 0.80–1.00, very high agreement.
All tests were 2-tailed, and P values < .05 were considered significant. Statistical analysis was performed using R statistical and computing software (http://www.r-project.org), SPSS (Version 24.0; IBM, Armonk, New York), and MedCalc for Windows (Version 15.2.0.0; MedCalc Software, Mariakerke, Belgium).
Results
Seventy-two patients were evaluated, with 2 patients in the case group excluded because of poor image quality (poor contrast). Thus, 70 patients were included in the final analysis. The mean age of the sample was 48.3 ± 18.9 years (range, 2–84 years), and 57.1% were men. Forty-eight patients in the case group were diagnosed with BD. By contrast, 22 patients in the control group were candidates for thrombolysis to treat ischemic stroke. The patients in the case group were comparatively younger (44.0 ± 18.6 versus 57.6 ± 16.4 years; P = .005), but no significant differences were found in sex between the groups (58.3% versus 54.5%; P = .766).
The initial causes of coma were aneurysmal subarachnoid hemorrhage (n = 17, 35.4%), head trauma (n = 13, 27.1%), cerebral hemorrhage (n = 5, 10.4%), brain tumor (n = 4, 8.3%), ischemic stroke (n = 4, 8.3%), and gunshot wound (n = 2, 4.2%). Three other cases (6.3%) involved hydrocephalus due to ventriculoperitoneal shunt malfunction, hypoxic-ischemic encephalopathy after cardiorespiratory arrest due to respiratory causes, and a postoperative complication of Chiari malformation type I. Twenty-six patients presented with SDs (16 craniotomies and 10 craniectomies). The median time interval between the final declaration of BD and CTA was 641 minutes (interquartile range, 269–883 minutes). Stratified analysis according to the presence and type of SD indicated no significant differences in age, sex, BD etiology, or the time interval between the declaration of BD and CTA. None of the patients in the control group had an SD (Table).
Characterization of the groups according to the presence and type of skull defecta
The 48 included patients in the case group were stratified according to the presence and type of SD. CTA demonstrated brain circulation arrest, defined according to the criteria of Frampas et al,12 in 41 patients (41/48; sensitivity: 85.4% [95% CI, 72.2–93.9]). Among those with an intact skull, CTA was consistent with BD in 21 patients (21/22; sensitivity: 95.5% [95% CI, 77.2–99.9]). For those with an SD, CTA was consistent with BD in 20 patients (20/26; sensitivity: 76.9% [95% CI, 56.4–91.0]). The patients with an SD were subdivided into the craniotomy and craniectomy groups. CTA was consistent with BD in 14 patients with craniotomy (14/16; sensitivity: 87.5% [95% CI, 61.7–98.5]) and 6 patients with craniectomy (6/10; sensitivity: 60.0% [95% CI, 26.2–87.8]). The categorization of patients with BD according to the criteria of Frampas et al,12 is summarized in Fig 1.

Flow chart of patients with a clinical diagnosis of brain death who underwent a CTA protocol proposed by Frampas et al,12 according to the presence and type of skull defect. Application of the interpretation criteria of the images proposed by Frampas et al.
SF was diagnosed in 28 patients (28/45, 62.2%). Among these, 11 patients (11/20, 55.0%) had an intact skull, 10 patients (10/15, 66.7%) had undergone craniotomy, and 7 patients (7/10, 70.0%) had undergone craniectomy (P = .390).
Seven patients (7/48 = 14.6%) did not have a BD diagnosis from CTA using the criteria proposed by Frampas et al.12 Among these, 5 patients (5/7, 71.4%) presented with SF (P < .001) and 2 patients (2/7, 28.6%) with craniectomy presented with arterial opacification of the distal branches (M4) in the arterial (early) acquisition of CTA. The false-negative CTA results were due to the SF phenomenon in 1 patient (1/20, 5.0%) with an intact skull, 2 patients (2/15, 13.3%) with craniotomy, and 2 patients (2/10, 20.0%) with craniectomy (P = .208) (Fig 2).

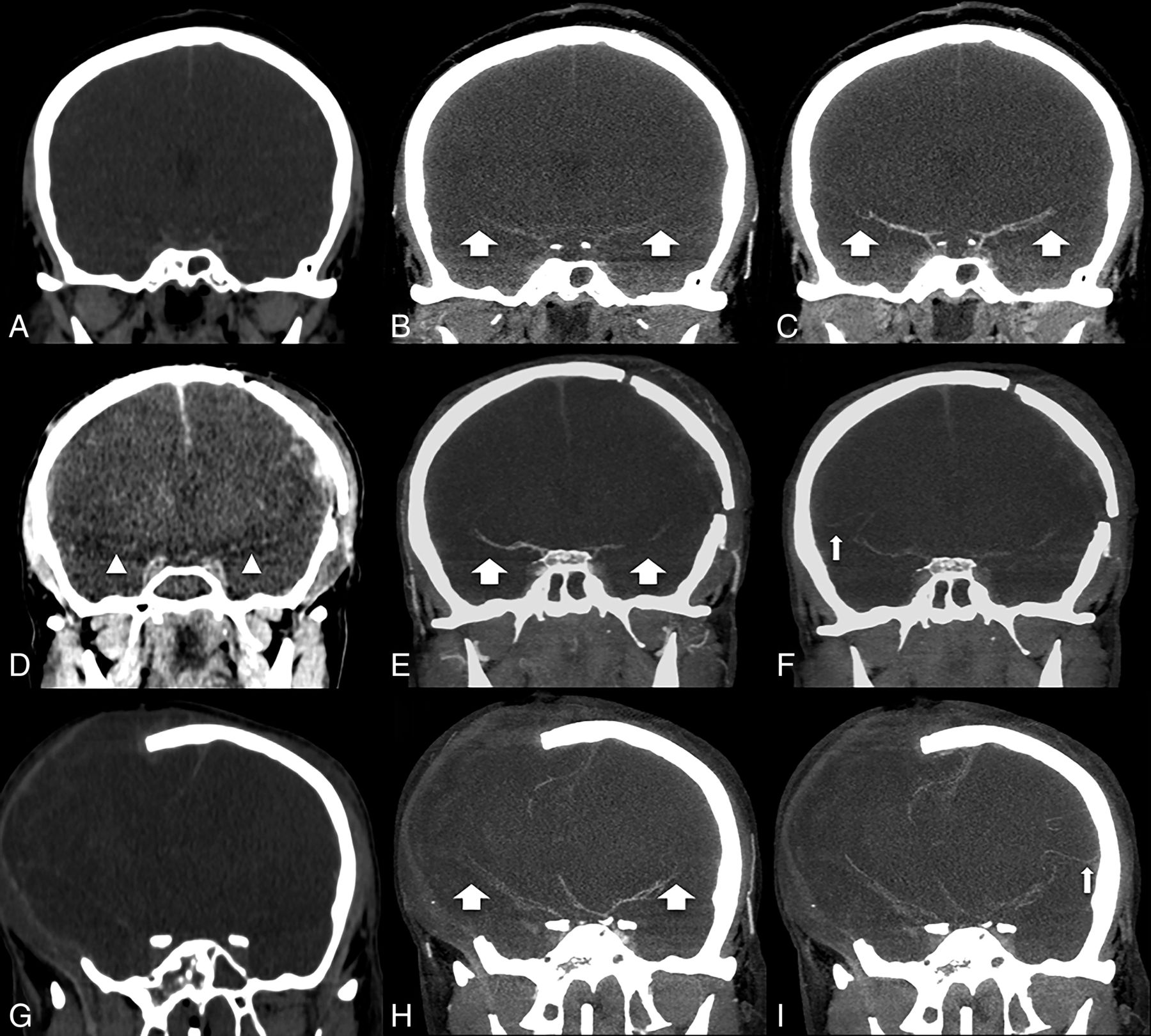
Comparison of CT images without contrast medium (A, D, and G) in the arterial (B, E, and H) and venous (C, F, and I) phases of CTA (MIP reformations in coronal plane) from 3 distinct patients with a brain death clinical diagnosis. In a patient with an intact skull (upper row, A–C), opacification was observed in the M1–M2 branches (broad arrows) in the arterial (B) and venous (C) phases and was more intense in the late phase. In a patient with craniotomy (middle row, D–F), one can appreciate the relative hyperattenuation of both M1 branches mimicking vascular opacification in noncontrast CT (arrowheads in D). Opacification was observed in both M2 branches (broad arrows in the arterial phase, E) and the right M3 branch in the venous phase (thin arrow in F), a phenomenon known as stasis filling. In a patient presenting with craniectomy (lower row, G–I), opacification was observed in both M2 branches (broad arrows in the arterial phase, H), the right M3 branch, and the left M4 branch in the venous phase (thin arrow in I) due stasis filling, a false-negative case of BD.
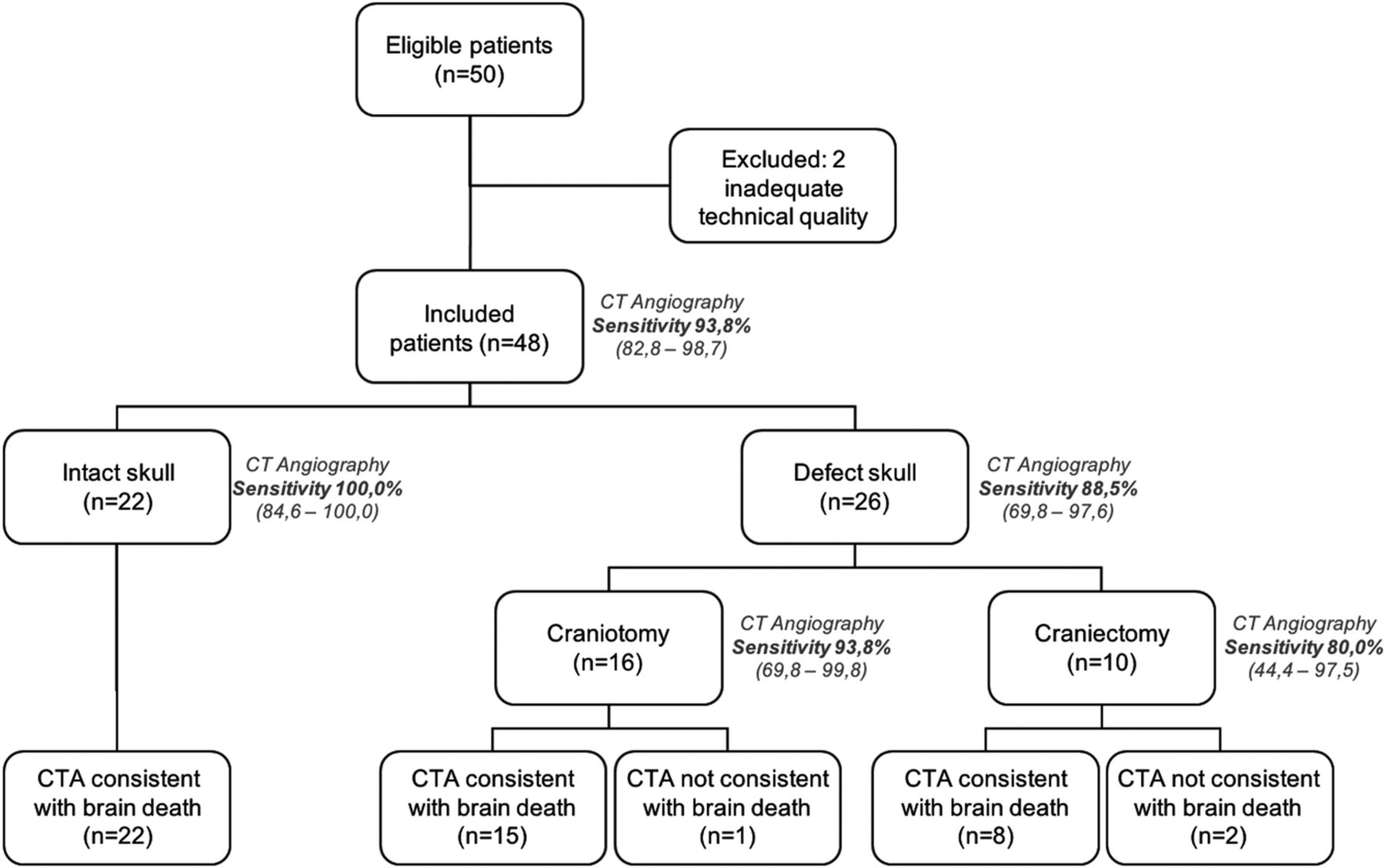
However, when the so-called modified Frampas criteria were applied, CTA demonstrated brain circulatory arrest in 45 patients (45/48; sensitivity: 93.8% [95% CI, 82.8–98.7]). Among those with an intact skull, CTA was consistent with BD in 22 patients (22/22; sensitivity: 100.0% [95% CI, 84.6–100.0]). For those with an SD, CTA was consistent with BD in 23 patients (23/26; sensitivity: 88.5% [95% CI, 69.8–97.6]). The patients with an SD were subdivided into the craniotomy and craniectomy groups. CTA was consistent with BD in 15 patients with craniotomy (15/16; sensitivity: 93.8% [95% CI, 69.8–99.8]) and 8 with craniectomy (8/10; sensitivity: 80.0% [95% CI, 44.4–97.5]). The categorization of patients with BD according to the modified Frampas criteria is summarized in Fig 3.

Flow chart of patients with a clinical diagnosis of brain death who underwent the CT angiography protocol proposed by Frampas et al, according to the presence and type of skull defect. Application of the interpretation criteria of the images of the modified Frampas criteria.
Even with these modified criteria, 3 patients (3/48, 6.2%) did not have a BD diagnosis using CTA. These patients with false-negative findings of BD presented with arterial opacification of the distal branches (M4) in the arterial (early) acquisition of CTA: 1 patient (1/3, 33.3%) with craniotomy and 2 patients (2/3, 66.6%) with craniectomy.
There was a significant trend (P = .037) toward higher false-negative rates with more extensive SDs. Only 1 patient with craniectomy (1/45, 2.2%) showed opacification of the M4 branches and ICV in the arterial and venous series, respectively; in both, CTA criteria for BD were analyzed.
No association was found between the false-negative results and time interval between the diagnosis of BD and performance of CTA. The median time was 704 minutes (interquartile range 247–1157 minutes) among the cases with an incorrect diagnosis by CTA and 641 minutes (interquartile range 270–857 minutes) among the cases with a correct diagnosis (P = .405). Moreover, the percentage of incorrect diagnoses by CTA did not differ significantly among the time quartiles: first quartile, 93–270 minutes (2/12, 16.7%); second quartile, 270–641 minutes (1/13, 7.7%); third quartile, 641–857 minutes (1/11, 9.1%); fourth quartile, 857-1577 minutes (3/12, 25.0%) (P = .551). These results indicated that the accuracy of CTA is not affected by the time between the diagnosis of BD and the performance of CTA.
The specificity of CTA to confirm BD was 100% in patients with an intact skull—that is, no false-positive cases were found. The specificity in patients with SDs could not be estimated because the control group included no patient with an SD. There were no disagreements in the CTA analysis among the evaluators, resulting in a perfect Cohen κ of 1.0.
Discussion
Despite the heterogeneity of protocols from CTA to confirm BD, the scientific literature has confirmed that CTA is a reliable, safe, fast, accessible, less invasive, reproducible, and auditable alternative ancillary confirmatory test in patients with the clinical criteria of BD.12⇓⇓⇓⇓–17,27⇓⇓⇓⇓⇓–33 CTA has become increasingly common in the diagnosis of cerebral circulatory arrest and has already been licensed for use in many countries, such as Canada, Austria, Switzerland, France, the Netherlands, and Croatia.34
Frampas et al12 demonstrated the occurrence of cerebral circulatory arrest using CTA with moderate sensitivity (85.7%) and high specificity (100%), both by the absence of M4 branch and ICV opacification. Our study confirmed the reproducibility and diagnostic accuracy of CTA using the same criteria of 4 points proposed by Frampas et al,12 with a similar sensitivity (85.4%), positive predictive value of 100%, and absence of disagreement in the CTA analysis among the evaluators.
As Leclerc et al30 described and later studies have confirmed,13,31 the absence of ICV opacification constitutes the earliest and most sensitive (98.1%) finding to confirm the diagnosis of BD with CTA.12 Our study also corroborated the high sensitivity (97.98%) of the absence of ICV opacification. However, the exclusive evaluation of the intracranial venous compartment for the diagnostic documentation of BD with CTA should be made with caution, particularly among patients with intracranial hypertension, possibly reducing the specificity of the method. Moreover, the occurrence of deep cerebral venous thrombosis should always be considered to avoid possible false-positive results.
The protocol for BD diagnosis advocated by Frampas et al12 includes image acquisitions of NCCT and biphasic CTA. Alternatively, Sawicki et al18 proposed optimizing the CTA technique by performing a single series with an acquisition delay of 40 seconds after the initiation of intravenous ICM infusion. Our study indicated that the maximum progression of the ICM in the intracranial vascular bed occurs during the late acquisition of CTA (venous phase), particularly among patients with concurrent SDs. However, the isolated evaluation of the late phase of CTA potentially limits the differentiation of spontaneously hyperattenuating vascular content, which was often found in our patients with extensive intra- and extracranial edema (pseudo-subarachnoid hemorrhage versus true vascular opacification) because of the SF. This study reinforces the importance of the protocol proposed by Frampas et al12 to avoid mistakes in diagnostic interpretation, thereby enabling comparisons between early and late acquisitions and providing reliable information for the correct evaluation of vascular opacification. The optimization of the interpretation criteria of the images proposed by Frampas et al12 called the modified Frampas criteria, which consist of the absence of opacification of the M4 branches in the arterial phase and ICV in the venous series of the CTA, decreased the number of patients with false-negative findings due to a reduced influence of SF (which is usually present in the arteries during the venous phase), particularly with an SD.
Hemodynamic changes resulting from an SD might represent a confounding factor in the context of BD,10,22 thereby necessitating detailed studies to define the limits of the interpretation for clinical purposes. Two distinct scenarios have been associated with the occurrence of false-negative results during the confirmation of BD in CTA studies: concomitant SD and acute hypoxic-ischemic encephalopathy after cardiorespiratory arrest.12,13,18,22,23,34 Our study confirmed that patients with an intact skull had high sensitivity and specificity for confirming BD by CTA, especially when the modified Frampas criteria were used for interpretation of the images, with results similar to those of conventional angiography (the criterion standard). There is a tendency for diagnostic errors to confirm BD by CTA (false-negative results) in patients with DS, particularly craniectomy, when the interpretation criteria of the images of Frampas et al12 were used, probably because of lower intracranial pressure.35⇓–37
First described in studies involving conventional angiography,10,26 the weak, slow, persistent, and progressive opacification of the intracranial arterial branches by ICM is known as SF.26 This finding stems from the progression of intravascular ICM in a high-resistance distal vascular bed without the ability to perfuse the brain parenchyma.13,15,38 Recent studies using CTA have indicated a high prevalence of this finding, varying between 45% and 59% of all patients with confirmed BD.17,29,38 The present results indicated an intermediate rate (62.2%) of SF in the total sample when the criteria of Frampas et al12 were used for interpretation of the images. The incorrect diagnosis of BD by CTA was meaningly more common in patients with SF. Despite the small number of cases, this problem tends to occur more frequently in patients with SDs, especially those who have undergone craniectomy, with or without opacification of the venous compartment including the ICV. The interpretation of the images according to modified Frampas criteria decreased the false-negative results and diagnostic mistakes.
Limitations of the present study include intracranial pressure not being measured; thus, establishing quantitative correlations with imaging findings was prevented. CTA to confirm BD also presented some drawbacks, such as the transportation of patients with hemodynamic instability and the difficulty of peripheral venous access in patients with edema.
Strategies to increase the accuracy of CT as a whole in the diagnosis of BD, which might be the object of future studies, include the use of CTP in addition to the standard protocol. CTP is a promising evidentiary method, given the increasing technologic development, the availability of equipment with higher temporal and spatial resolution, and reduced intravenous ICM use. However, some variations in the use of this technique demand the establishment and validation of new standard CTP protocols.
Conclusions
This study showed that that the CTA protocol proposed by Frampas et al12 has high sensitivity and reproducibility, as well as perfect specificity and interobserver agreement, for BD confirmation in patients with an intact skull. The optimization of the interpretation of the images according to the modified Frampas criteria increased the sensitivity of the CTA, particularly in patients with SDs. No control case was wrongly diagnosed as BD. These data add to the growing medical literature supporting the use of CTA as a reliable ancillary BD test. A concurrent SD, particularly craniectomy, can decrease the sensitivity of CTA for BD confirmation, mainly due to the SF phenomenon. The evaluation of CTA images according to the modified Frampas criteria reduced false-negative findings, especially with craniectomy. Negative results may arise in this clinical scenario, requiring the consideration of other corroborating tests to confirm BD in patients with SD.
Acknowledgments
We extend our appreciation to the Organ Procurement Organization, Santa Casa de Misericordia de São Paulo Hospital, São Paulo, Brazil. The authors thank the institutional publishing support center (Núcleo de Apoio a Publicação) for technical assistance in publication.
REFERENCES
- Received March 2, 2019.
- Accepted after revision May 13, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.