
Abstract
BACKGROUND AND PURPOSE: Strong emphasis has been placed recently on early (4 postnatal months) detection of tuberous sclerosis complex and the introduction of antiepileptic treatment before seizure onset. This objective can be achieved prenatally: Cardiac rhabdomyomas and the major diagnostic tuberous sclerosis complex sign are detected during fetal ultrasound, and prenatal MR imaging allows detection of cerebral major manifestations: cortical tubers, subependymal nodules, and subependymal giant cell astrocytomas.
MATERIALS AND METHODS: We retrospectively reviewed 50 fetuses with ultrasound-detected cardiac tumors at 19–36 gestational weeks (median, 31 weeks). MR imaging with the use of 1.5T scanners was performed at 24–37 gestational weeks (median, 34 weeks).
RESULTS: In 11 fetuses (22%), cardiac tumors remained the only criterion. In remaining 39 fetuses (78%), MR imaging revealed a prenatal diagnosis of tuberous sclerosis complex, having shown an additional 1–3 major criteria: subependymal nodules in all cases (39/39 = 100.0%), subependymal giant cell astrocytomas in 6 (6/39 = 15.4%), and cortical tubers in 24 (24/39 = 61.5%). Radial migration lines and cerebellar tuber, not published so far, were shown in 1 case each.
CONCLUSIONS: A schedule of proper care of children with tuberous sclerosis complex can be established during the perinatal period due to education of women to report for mandatory ultrasound examinations during pregnancy, the good quality of ultrasound, and referral to MR imaging if a cardiac tumor is depicted on ultrasound. Gynecologists and pediatric cardiologists performing fetal ultrasound and radiologists performing prenatal MR imaging are a key to early diagnosis of tuberous sclerosis complex in many cases.
ABBREVIATIONS:
- CT
- cortical tuber
- GW
- gestational week
- SEGA
- subependymal giant cell astrocytoma
- SEN
- subependymal nodule
- SSFSE
- single-shot fast spin-echo
- TSC
- tuberous sclerosis complex
- US
- ultrasound
Epileptogenesis in tuberous sclerosis complex (TSC) starts prenatally with epilepsy, according to some authors, in 100% of TSC cases. In recent years, there has been strong emphasis on the early detection of TSC and on the early introduction of antiepileptic treatment before the seizure onset to improve the neurodevelopmental outcome of the affected children. In neurological journals, “early” means the first 4 months (16 weeks) of postnatal life because this time point is regarded as the usual time of clinical seizure onset.1
It is estimated that up to 90% of children with cardiac rhabdomyomas have TSC, at least 50% of children with TSC have cardiac rhabdomyomas, and almost 100% of fetuses with multiple rhabdomyomas have TSC.2 Rhabdomyomas are the most common type of fetal primary cardiac tumors, with an incidence of 60%3 to 86%.4 They are detected during fetal ultrasound (US) with further characterization on fetal echocardiography.
Being 1 major diagnostic sign of TSC, cardiac rhabdomyomas require the second major feature to confirm the diagnosis. Prenatal MR imaging allows detection of cerebral TSC manifestations. These are cortical tubers, subependymal nodules (SENs), and subependymal giant cell astrocytomas (SEGAs).
If one takes the above into account, a big percentage of patients could be diagnosed prenatally by cardiac rhabdomyomas and brain lesions, which is much earlier than the first 4 months of postnatal life. If the diagnosis is confirmed by 2 major signs, an optimal perinatal strategy can be introduced.
On the basis of the experience of 2 tertiary diagnostic centers (Department of Diagnostic Imaging, Institute of Mother and Child, and Referral Center for Fetal Cardiology, Agatowa Sonography Clinic, Warsaw, Poland), the authors show that an early diagnosis of TSC means a prenatal diagnosis, which is feasible in the experienced hands of fetal cardiologists and radiologists. Also, the recent publication in the American Journal of Neuroradiology, presenting 47 published cases from PubMed and 4 cases of the authors, prompts us to publish our material.5
MATERIALS AND METHODS
The study group consisted of 50 retrospectively reviewed fetuses with cardiac tumors detected on US and referred to MR imaging, with a diagnosis of cardiac tumors suggestive of rhabdomyomas to confirm or rule out TSC. Informed consent for clinical investigations was obtained from all patients. The Bioethical Committee's approval was waived due to the retrospective character of this study.
There were 5 fetuses with 1 cardiac tumor, 29 fetuses ≥2 cardiac tumors, and in 16 fetuses, the number of cardiac tumors was unclear (missing an exact US report and images, cardiac tubers known from the referral sheet and from MR images). In the second group, in 2 cases, we dealt with a dichorionic diamniotic pregnancy of a mother with TSC with only 1 fetus affected and a healthy co-twin. Cardiac tumors were detected on US between the gestational ages of 19 and 36 weeks (median, 31 weeks), and MR imaging was performed between 24 and 37 gestational weeks (GWs), median, 33 GWs.
In 32 cases, US was performed in the Referral Center for Fetal Cardiology, Agatowa Sonography Clinic. Each fetus had detailed fetal echocardiography using the Voluson Expert (GE Healthcare) or EPIQ7 (Philips Healthcare) machines.
MR imaging was performed without maternal and fetal sedation with the use of a 1.5T scanner in single-shot fast spin-echo (SSFSE)/T2- and FSE/T1-weighted images (and/or 3D T1 LAVA-Flex; GE Healthcare), FIESTA/2D, gradient-echo EPI, and DWI sequences in 3 planes. Details of MR imaging protocol are shown in Table 1.
Details of MR imaging protocol
RESULTS
Among the group of 50 fetuses, in 11 cases (22%), cardiac tumors remained the only criterion of TSC, and the suspicion of TSC was not confirmed on fetal MR imaging. Of these 11 cases, in 3, there were single cardiac tubers; in 3, cardiac tubers were multiple; and 5 belonged to the group with an unclear number of cardiac tumors. In the remaining 39 fetuses (78%), MR imaging allowed the prenatal diagnosis of TSC after having shown an additional 1–3 major criteria and in 2 cases, 1 minor criterion (multiple renal cysts) as well. These data are presented in Table 2.
Number of diagnostic TSC criteria in the analyzed material
SENs were detected on MR imaging in all cases of TSC (39/39 = 100.0%) and were not detected on US. In 6 fetuses (6/39 = 15.4%), SEGAs were diagnosed on MR imaging on the basis of their location near the foramen of Monro and a size of >10 mm, and in half of these cases, there was already asymmetric ventriculomegaly on the side of the tumor. Cortical tubers were the only cerebral manifestation of TSC suspected on US in 6 cases and confirmed on MR imaging in 5. Cortical tubers were found on MR imaging in 24 cases (24/39 = 61.5%). In one of these cases, we could also observe migration lines on MR imaging.
The SSFSE/T2-weighted sequence was the most important one for making the diagnosis of cerebral manifestations of TSC: SENs, SEGAs, and cortical tumor (CTs) with clear hypointensity of these lesions most strongly expressed in the case of SENs and SEGAs, which were the most conspicuous lesions. Their visualization was weaker on FIESTA/2D. Gradient recalled-echo EPI was used to differentiate SENs from foci of germinal matrix/subependymal hemorrhage and calcifications. CTs were more difficult to diagnose due to weaker delineation from the surrounding brain tissue and weaker hypointensity on SSFSE/T2. It was particularly important in cases of CTs to perform and compare SSFSE/T2, FIESTA/2D, and T1-weighted images. The latter, which are always inferior in fetal studies, were, nevertheless, helpful, showing the (weak) hyperintensity of these lesions.
Failure to see SENs in at least 2 projections or the questionable images of CTs were treated as the absence of the second major criterion, and TSC was not confirmed; while on the other hand, the obvious image of SENs in at least 2 planes was a clear second major criterion, allowing a reliable prenatal diagnosis of TSC.
Detailed information on the TSC criteria detected in the study group on US and MR imaging is presented in Table 3.
Details of US and MR imaging findings in the analyzed material
Single renal cysts were found on MR imaging in 2 fetuses and, for obvious reasons, were not regarded as a diagnostic criterion. Multiple renal angiomyolipomas were detected in mothers in 2 cases.
DISCUSSION
Subependymal nodules, subependymal giant cell astrocytomas, multiple cortical tubers and/or radial migration lines, and cardiac rhabdomyomas are the major features of TSC as listed in the updated diagnostic criteria for TSC in 2021. Brain abnormalities are the domain of MR imaging, and cardiac ones are diagnosed on US, and it is possible to detect them in the prenatal period. Two major features are sufficient to make a definite diagnosis of TSC,6 and 2 diagnostic methods (fetal US and MR imaging) are necessary to reach this diagnosis, also before birth. In the PubMed database, we found the first description of a prenatal diagnosis of TSC on MR imaging dating back to 1992.7 Our interest in this topic has also been ongoing for years, with the first publication in 2007.8
Neuroimaging findings of SENs, SEGAs, and what was formerly called cortical dysplasia are often identified after an initial presentation, but we strive for an early diagnosis in this considerable group of patients whose brain involvement occurs early in fetal life. In an article by Davis et al,9 35% of 130 infants with TSC presented prenatally. It is, therefore, a large group, and it is worth fighting for an early diagnosis in this group of patients.
An early diagnosis should be reached in these cases, provided that pregnant women are required to present themselves for US during gestation. Having found cardiac tubers, a fetal US specialist should refer the expectant mother to MR imaging for a detailed assessment of the brain. This referral is to answer the question, “How to make the diagnosis before seizures.”1 It is what experts have advised since at least 2014,10 and this procedure is followed by the authors' 2 centers.
Incidentally, seizures may begin before birth, not only in association with TSC. They may be felt by the mother and confirmed on US11 or on MR imaging, especially in the cine mode. In our material, one pregnant woman with prenatally confirmed TSC reported the recent change of her baby's movement pattern, with a new onset of rhythmic, repetitive movements lasting for several seconds which, though not visualized during MR imaging, most likely represented seizures.
There are several questions: 1) Is it possible to diagnose specifically cardiac rhabdomyoma? 2) Is it possible to diagnose, specifically, SENs, SEGAs, and cortical dysplasia prenatally?
Cardiac rhabdomyomas are quite easy to detect during fetal echocardiography. They usually occur in the third trimester of pregnancy, so most of them cannot be seen during the US, which is performed around 20 weeks of gestation. The US appearance of rhabdomyomas is very characteristic (Fig 1A–D). They are histologically benign; however, they are a typical sign of TSC. It is important to check their location because sometimes they obstruct inflow or outflow of the heart. Although they occur very rarely, they are a life-threatening condition for neonates, so perinatal specialist care should be instituted.

Typical echocardiographic images of multiple cardiac tumors (rhabdomyomas) in 3 different fetuses (fetus 1, 38 GWs (A); fetus 2 (B), 35 GWs; fetus 3 (C and D). A and B, Tumors are located in both ventricles and attached to the ventricular walls and interventricular septum and do not disturb blood flow. C and D, A huge cardiac tumor located in the RV, compressing the LV, and disturbing blood flow through both ventricles (C, 2D view; D, 3D view). E, MR imaging at 30 GWs. SSFSE/T2-weighted image, coronal plane: hypointense cardiac tumor (arrow) against the background of the “black hole” of a heart. RV, right ventricle; LV, left ventricle; Ao, aorta; T and/or * tumor.
Cardiac rhabdomyomas have a quite typical appearance on US. They are usually firmly attached to the heart muscle, interventricular or free ventricular walls, rarely in the atria. They are always oval and have various sizes, from a few millimeters to the huge tumor that involves most of the cardiac cavity. Most commonly, their diameter is a few millimeters, and they do not disturb blood inflow or outflow. They look slightly more hyperechogenic than the heart muscle.
On MR imaging, cardiac rhabdomyomas are uniformly hyperintense on SSFSE/T2-weighted images against the background of a dark heart that is called a “black hole” (Fig 1E). Being the most common cardiac tumors in the prenatal period, often multiple, they usually do not cause diagnostic uncertainty.
SENs are occult to US and are detected only on MR imaging in most cases. These nodules are T2-hypointense (Fig 2) and, according to the literature, display typically bright signal on T1-weighted images.12,13 The latter was not obvious in our experience, most likely due to the suboptimal quality of T1WI and the small size of these nodules. SENs should not be diagnosed unless they are demonstrated in 2 different projections, eg, axial and coronal, to avoid misdiagnoses. The differential diagnosis of SENs on fetal MR imaging includes subependymal heterotopia and subependymal hemorrhage.12 Nagaraj et al14 added to this list abnormal nodularity of the germinal matrix that does not correspond to subependymal heterotopia postnatally. The normal germinal matrix that forms on the ventricular walls is smooth and symmetric. During development in utero, it increases in volume between 13 and 26 GWs, then loses half of its volume between 26 and 28 GWs, and decreases further thereafter. Between 26 and 28 GWs, the germinal matrix is at high risk of hemorrhage.13 However, subependymal hemorrhage is often associated with ventricular bleeding, detected on US, and has a typical evolution on follow-up US.12 The nodular appearance of the ventricular walls that is depicted on MR imaging early in pregnancy, eg, at 21 GWs, suggests subependymal heterotopia; late appearance in the third trimester is more suggestive of SENs in TSC. In our study group, SENs were detected on prenatal MR imaging in 78% of cases in all fetuses with prenatally diagnosed TSC and represented the second major criterion in all cases of TSC. They were not described on US in any fetus in our study group.

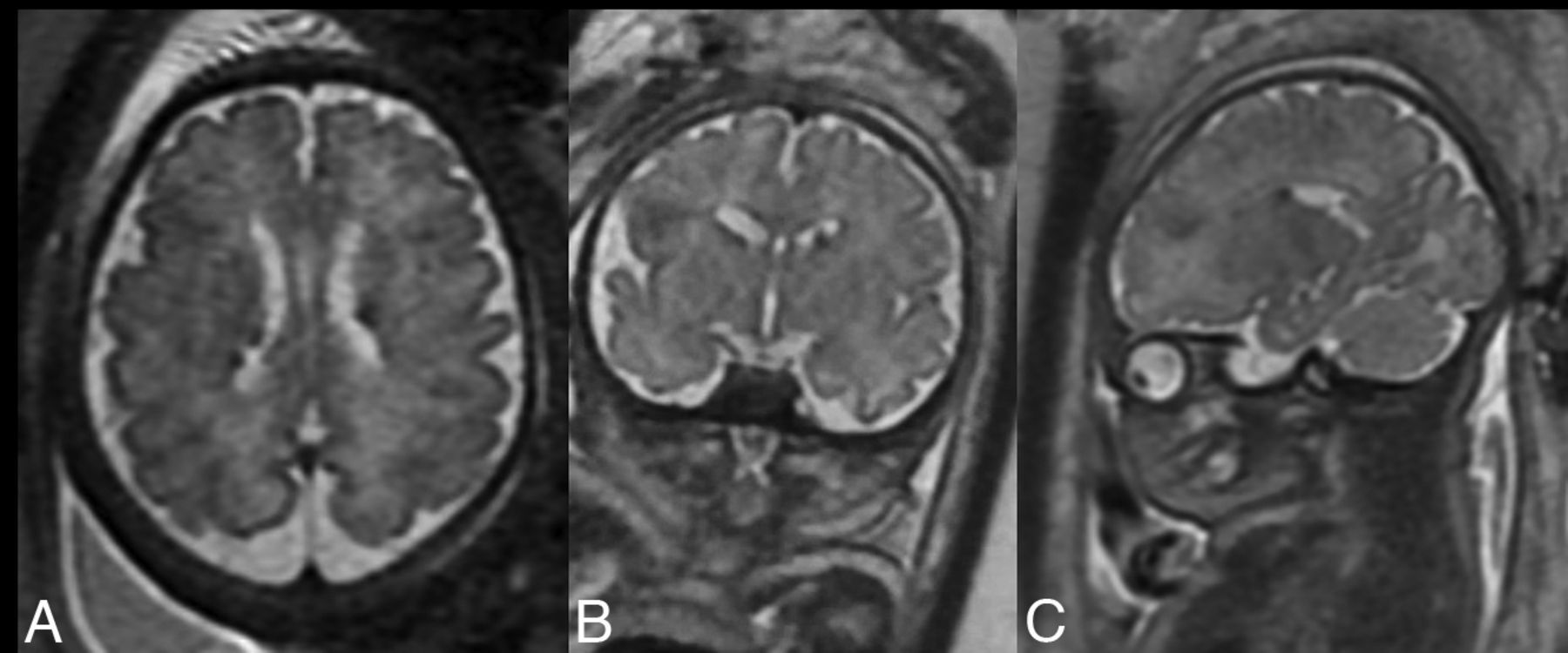
T2-hypointense subependymal nodules on the axial (A), coronal (B), and sagittal (C) planes.
SEGAs also belong to the list of major features of TSC. They have an incidence of 5%–15% in TSC and tend to arise from SENs later in life, though they may also be detected prenatally. Their most common location is near the foramen of Monro; thus, they can cause obstructive hydrocephalus.6 The definition of SEGA is as follows: a tumor at the caudothalamic groove of >10 mm in any direction or any SEN that had demonstrated growth across consecutive imaging studies.15 The first part of this definition was used in our study because only 1 fetus with a TSC diagnosis had the second MR imaging performed (and no progression of the SEGA was noted during a 4-week period). SENs of <10 mm located near the foramen of Monro were found in 20 cases in our material, and SEGAs, in as many as 6 (Fig 3A–C).
In the published report on the prenatal diagnosis of SEGA by Hussain et al,16 there were no dimensions of the tumor reported, but it was huge. Kotulska et al17 reported 2 cases of a prenatal diagnosis of SEGAs in their material but did not show the images and did not address the question of the dimensions of the tumor and growth and hydrocephalus; therefore, it is unclear on what basis SEGAs were diagnosed in these 2 cases. Most interesting, these authors reported in their retrospective study that only 10 of 452 (2.2%) patients with TSC were diagnosed with SEGA in the first 3 months of life, while in our, much smaller material, this percentage is much higher, only in the prenatal period (15.4%).
Finally, cortical tubers, which constitute another major feature of TSC, were seen less frequently than SENs in the prenatal period on MR imaging. Similar to SENs, they are T2-hypointense and T1-hyperintense (Fig 3B, -D).18 In our material, they were present in 61.5% of cases of TSC. In the literature, cortical tubers are reported as the most frequent finding in the prenatal period;10 this was not confirmed in our material. In the newest updated TSC diagnostic criteria, the new criterion has been formulated as “multiple cortical tubers and/or radial migration lines,”6 and in our material, we have 1 case in which radial migration lines seem to be present as radial T2-hypointense lines (Fig 4A, -B). These lesions are described in the literature as displaying low signal intensity on T1-weighted images and high signal intensity on T2- and FLAIR; however, this MR imaging pattern is reversed in young infants (and fetuses) against the background of the surrounding unmyelinated brain with increased water content.18 No reports on radial migration lines on fetal MR imaging have been found in the literature. On the contrary, statements such as “white matter abnormalities were not evaluated in this study because of their poor visibility on fetal MR imaging” were noted.19 Most interesting, in our study, there is also 1 case of a cerebellar tuber that, in addition, has already been depicted on US and confirmed on MR imaging (Fig 4C, -D). No reports on cerebellar tubers on fetal MR imaging have been found in the literature either.

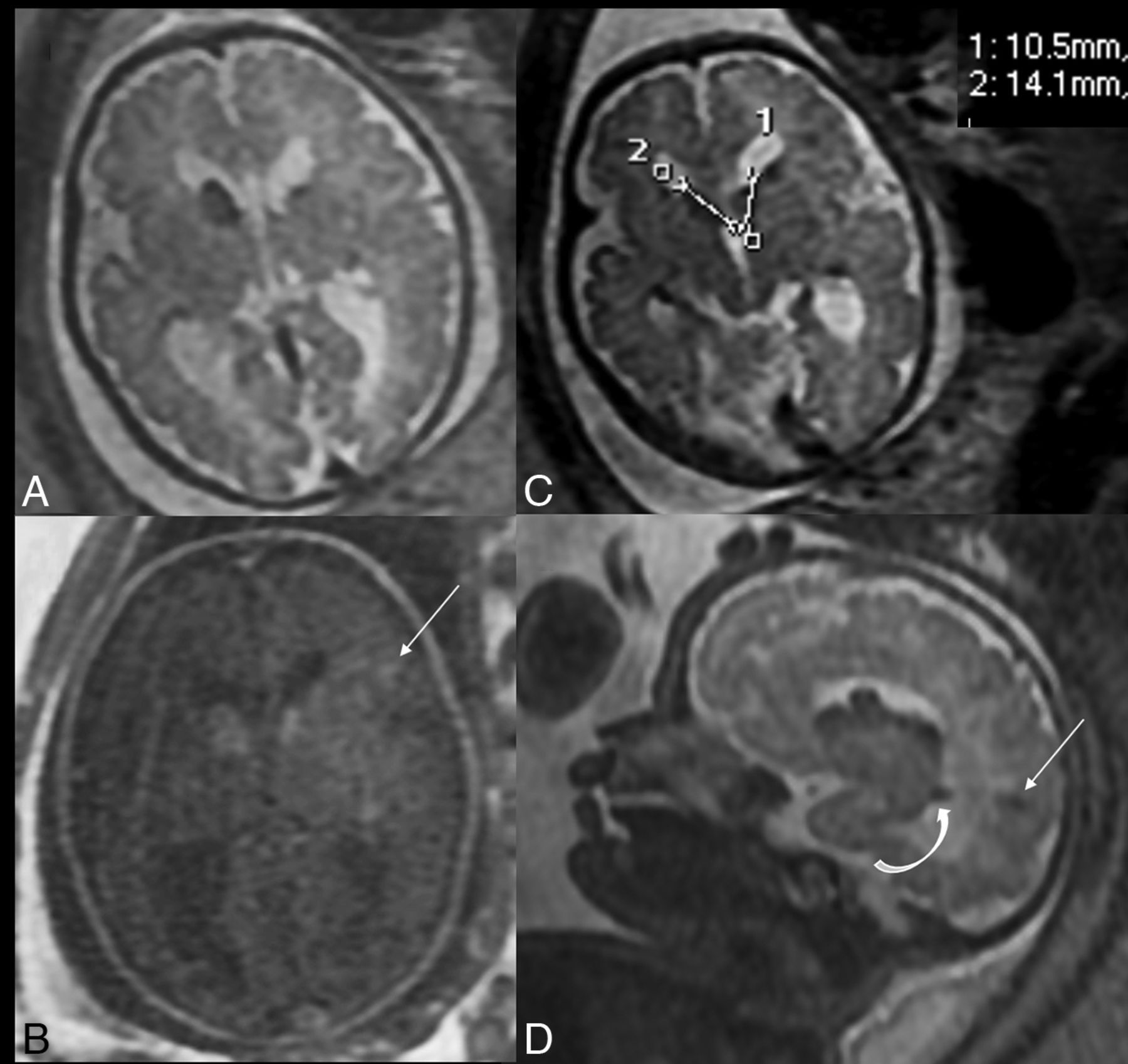
MR imaging at 32 GWs. SSFSE/T2-weighted images in the axial (A and C) and sagittal (D) planes and an axial T1-weighted image (B). A fetus with 4 major criteria: cardiac tumors (not shown here), 2 SEGAs (measured), SENs (curved arrow), and cortical tubers (straight arrows).

MR imaging of 2 different fetuses: at 35 GWs (A and B) and at 29 GWs (C and D). SSFSE/T2-weighted images. A and B, T2-hypointense radial migration lines. C and D, T2-hypointense tuber in the right cerebellar hemisphere.
We cannot agree with the recently published information that “cortical tubers are occasionally detected only on the postnatal MR imaging of the brain.”20 The authors of this article contradict themselves, writing a few lines earlier that US and MR imaging “indicate that cortical tubers and SENs are the most common lesions detected prenatally.” We cannot agree with another statement from this publication that “no significant difference was found in the time of detection” of “characteristic TSC brain lesions…comparing the two methods”: US and MR imaging. Again, it is a well-known and documented fact that brain lesions are often sonographically occult,21 and this fact was also shown in our study. Thus, despite a seemingly well-described topic and relatively extensive literature, there is still a need for research and publications on prenatal diagnosis of TSC.
In a prospective study conducted in Germany in 2015–2017 by Ebrahimi-Fakhari et al,22 in a group of 86 patients who had met the inclusion criteria of definite or possible TSC, the median age at diagnosis was 6 months (range, 5 months before birth to 197 months of age). Moreover, in the prenatal period only the diagnosis of possible TSC was established on US after cardiac rhabdomyomas had been detected in 22.1% of patients (19/86). Only one of these patients had “concomitant cerebral abnormalities” that were not further characterized and did not lead to the final diagnosis. In a retrospective French study by Saada et al,23 in turn, 25 of 51 fetuses with ≥1 cardiac tumor (49%) were diagnosed with TSC after fetal MR imaging. On the one hand, this finding illustrates the approach to prenatal diagnostics in general and to prenatal MR imaging in particular, and on the other hand, it indicates the quality of the diagnostics, both different in different countries.
In our material, all pregnant women with cardiac tumors diagnosed on US were referred to MR imaging. Major features of cerebral TSC were found in as many as 78% of the analyzed cases, confirming the diagnosis. In more than half of cases of TSC (22/39 = 56.4%), the fetuses showed >2 major TSC criteria that are necessary to establish the diagnosis (Fig 3).
In cases of inherited TSC, the features of maternal disease within the FOV of the fetal MR imaging may be helpful, ie, renal angiomyolipomas (Fig 5C).21 Angiomyolipomas are a major TSC diagnostic criterion but are not encountered prenatally. Multiple renal cysts constitute the minor feature of the TSC diagnostic criteria and are very rarely depicted in a prenatal period. In our material, we had only 2 fetuses with small renal cysts, which is consistent with findings in the literature.20

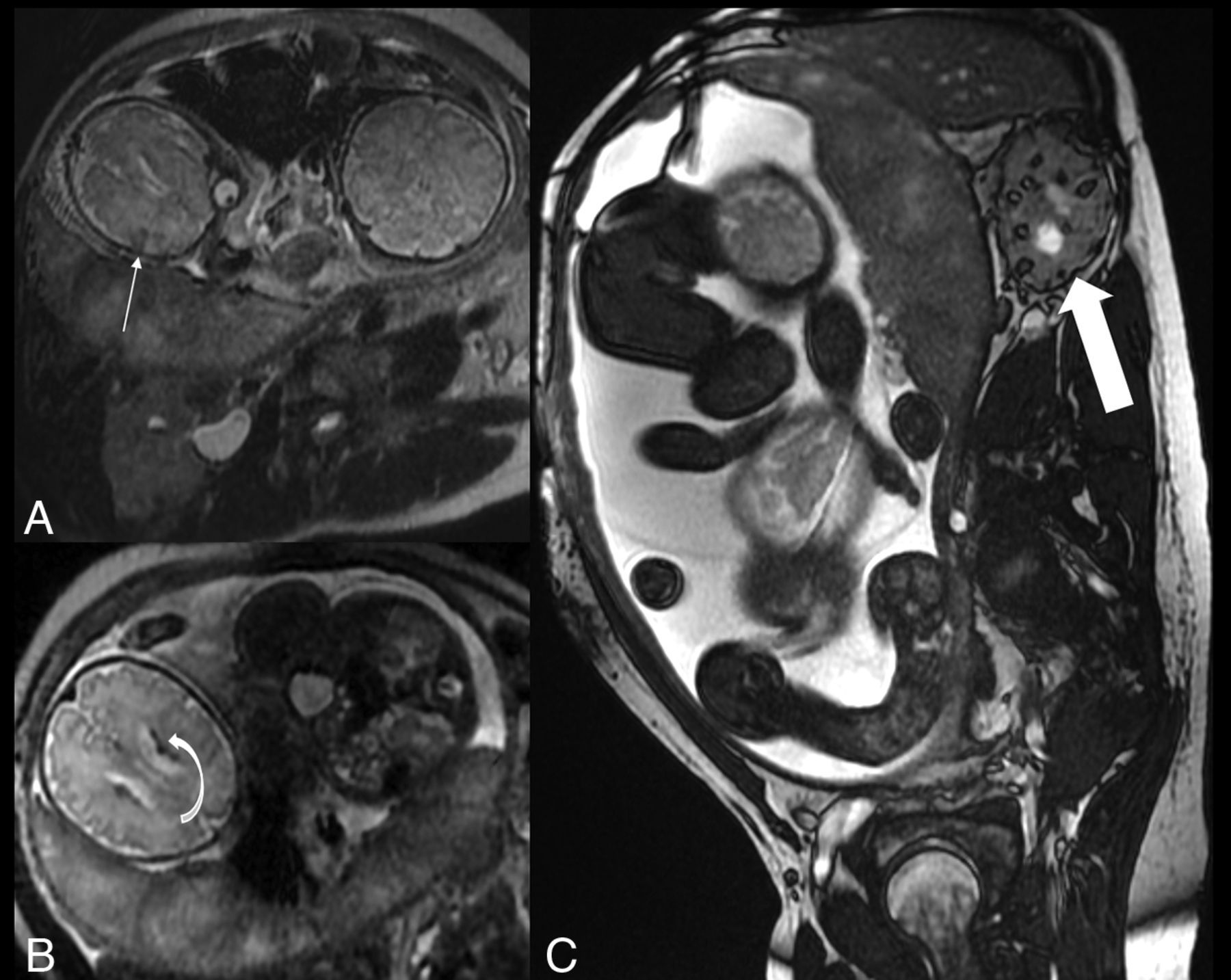
MR imaging at 34 GWs. SSFSE/T2-weighted images (A and B) and FIESTA (C). Dichorionic diamniotic pregnancy of a mother with TSC, with angiomyolipomas in the kidney (C, Thick arrow). Note the fetus on the left side of the images with a cortical tuber (A, Thin arrow) and SENs (B, Curved arrow).
It has been postulated since at least 2007 that TSC Consensus Conference criteria can and should be applied to fetal MR imaging and that this method should be better promoted.24 Then, the diagnosis could be established much earlier than within the first 4 months of postnatal life in a significant group of patients,1 a possibility that was shown in our material. In 2021, a group of experts working on TSC with the long-term, prospective study evaluating clinical and molecular biomarkers of epilptogenesis in a genetic model of epilepsy–tuberous sclerosis complex (EPISTOP) consortium finally admitted that “fetal cerebral MR imaging can be used reliably in the diagnosis of TSC.” The authors wrote as well that “to establish TSC prenatally, it is…necessary to detect another major feature of TSC” (meaning that cardiac rhabdomyomas are the first one) “or to confirm the diagnosis with DNA testing after amniocentesis.”19 The long-postulated recognition of prenatal MR images as sufficient to diagnose the disease has finally happened and will lead to a greater number of diagnoses at the right time. In this international multicenter retrospective study, 41 children with TSC who underwent prenatal MR imaging were included, a study group comparable with our material from only 2 centers.
CONCLUSIONS
The schedule of proper care of children with TSC can and should be established during the perinatal period in a large percentage of patients. It is necessary to emphasize the education of women to report on mandatory sonographic examinations during pregnancy, on the quality of US, and on the need to refer pregnant patients to MR imaging if a cardiac tumor is depicted on US. Gynecologists and pediatric cardiologists performing fetal US and radiologists performing prenatal MR imaging are the clue to the early diagnosis of TSC, before seizures in many cases, and many patients can win the race against time due to prenatal diagnostic imaging.
Footnotes
This work was supported by the internal grant of the Institute of Mother and Child, Warsaw, Poland, No. 510-14-03.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received March 28, 2023.
- Accepted after revision June 25, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.