
Abstract
BACKGROUND AND PURPOSE: Diffusion tensor imaging (DTI) was introduced as a good technique to evaluate structural abnormalities in the white matter. In this study, we used DTI to examine anisotropic changes of the pyramidal tracts displaced by chronic subdural hematoma (CSDH).
MATERIALS AND METHODS: Twenty-six patients with unilateral CSDH underwent DTI before and after surgery. We measured fractional anisotropy (FA) values in pyramidal tracts of bilateral cerebral peduncles and calculated the ratio of the FA value on the lesion side to that on the contralateral side (FA ratio) and compared the ratios with motor weakness. Moreover, the relationships between FA ratios and clinical factors such as age, sex, midline shift, interval from trauma, and hematoma attenuation on CT were evaluated.
RESULTS: FA values of pyramidal tracts on the lesion side were significantly lower than those on the contralateral side (0.66 ± 0.07 versus 0.74 ± 0.05, P < .0001). The FA ratio was correlated to the severity of motor weakness (r2 = 0.32, P = .002). FA ratios after surgery improved significantly compared with those before surgery (0.96 ± 0.08 versus 0.89 ± 0.07, P = .0004). Intervals from trauma and the midline shift were significantly associated with decreased FA ratios (P = .0008 and P = .037).
CONCLUSIONS: In patients with CSDH, a reversible decrease of FA in the affected pyramidal tract on DTI was correlated to motor weakness. These anisotropic changes were considered to be caused by a reversible distortion of neuron fibers and vasogenic edema due to the hematoma.
Chronic subdural hematoma (CSDH) is a progressive space-occupying lesion, which may lead to reversible reduction in cerebral function due to brain compression or brain displacement. The causes, clinical characteristics, and therapeutic management of CSDH are well established; however, the detailed physiology, including the mechanisms of appearance with motor dysfunction in patients, is still controversial.1–4
Diffusion tensor imaging (DTI) reveals the tissue microstructure and architecture of white matter tracts, including pyramidal tracts, and extracts the principal diffusivities, mean diffusivities (MD), and fractional anisotropy (FA). Previously, it was reported that decreased FA in the pyramidal tracts on DTI was associated with secondary degeneration and could be a reliable measure of motor weakness.5–8 The purpose of this study was to investigate changes of DTI in affected pyramidal tracts of patients with CSDH and to evaluate the association between changes of FA and clinical factors such as age, sex, hematoma thickness, midline shift, interval from the trauma, and attenuation on CT.
Materials and Methods
Study Populations
From September 2006 to February 2007, 26 consecutive patients (17 men and 9 women; age range, 44–90 years; mean, 78 ± 7.8 years; 15 right side and 11 left side; maximal width of hematoma, 21.4 ± 4.1 mm) with unilateral CSDH were examined by MR imaging 1–2 days before and 6–8 days after hematoma removal by burr-hole craniotomy (Table 1). In this study, we excluded patients with bilateral CSDH and patients who had pre-existing neurologic diseases such as cerebral infarction or hematoma. Seventeen of 26 patients had motor weakness, with the Manual Muscle Test (MMT)9 scores as follows: grade 2 (the patient has all or partial range of motion in the gravity-eliminated position) in 1 patient, grade 3 (the patient can tolerate no resistance but can perform the movement through the full range of motion) in 3 patients, and grade 4 (the patient can hold the position against strong-to-moderate resistance and has full range of motion) in 13 patients.
Patient details and clinical information
Immediately after burr-hole craniotomy, motor dysfunctions of 13 of 17 patients were drastically improved. The other 4 patients needed rehabilitation to be discharged from the hospital because of low-grade gait disturbance due to residual motor weakness (cases 5, 10, 18, and 21); these patients recovered within 2 weeks.
In comparison, 20 healthy volunteers (10 men and 10 women; age range, 13–74 years; mean, 54 ± 20 years) were examined by MR imaging in the same period. The study protocol was approved by the institutional review board, and informed consent was obtained from all patients.
MR Protocol
MR imaging was performed on a 3T MR imaging scanner (Signa Excite; GE Healthcare, Milwaukee, Wis) by using an 8-element phased-array neurovascular array coil. DTI was performed by using a single-shot echo-planar sequence with the array sensitivity–encoding technique. Motion-probing gradient orientations were applied along 15 directions, and the b factor was set at 1000 s/mm2. The acquisition parameters used were as follows: TR/TE, 12,000/70–76 ms; bandwidth, 143 kHz; matrix size, 128 × 128; section thickness, 3 mm without intersection gap; FOV, 30 × 30 cm; and NEX, 1. In addition, a reference image without diffusion weighting (b = 0 s/mm2) was obtained. In all patients and healthy volunteers, 50 sections were acquired parallel to the line of the nasofrontal angle and the pituitary fossa.
Image Analysis
One experienced neuroradiologist (M.M.), who was unaware of the neurologic status of the subjects, placed regions of interest 3 times in the anterior parts of the bilateral cerebral peduncle, which correspond to a pyramidal tract based on anatomic knowledge, of healthy volunteers and patients before and after surgery and measured and averaged the FA and MD values. Another experienced neurosurgeon (K.Y.) investigated the differences in FA and MD values between the right and left sides in healthy volunteers and between the lesion and the contralateral sides in patients before surgery (Fig 1).

A and B, Head CT and T2-weighted MR images of CSDH, respectively. C and D, Regions of interest in the bilateral pyramidal tract of the cerebral peduncle. C, FA map. D, Apparent diffusion coefficient map.
We calculated FA ratios (ratios of FA values in the lesion side/normal side) in the patients before surgery and investigated the correlation between the preoperative FA ratio and the presented motor weakness, which was classified by MMT. Furthermore, we analyzed the association between the preoperative FA ratio and clinical factors such as age, sex, hematoma thickness, midline shift, interval from the trauma, and attenuation on CT. Then we compared patients' FA ratios before and after surgery.
Statistical analyses were performed with the Wilcoxon signed rank test and a linear regression analysis by using StatView 5.0 software (SAS Institute, Cary, NC).10 All data are presented as means ± SD, and differences were considered statistically significant at a P value < .05.
Results
Patients' characteristics of this series are summarized in Table 1.
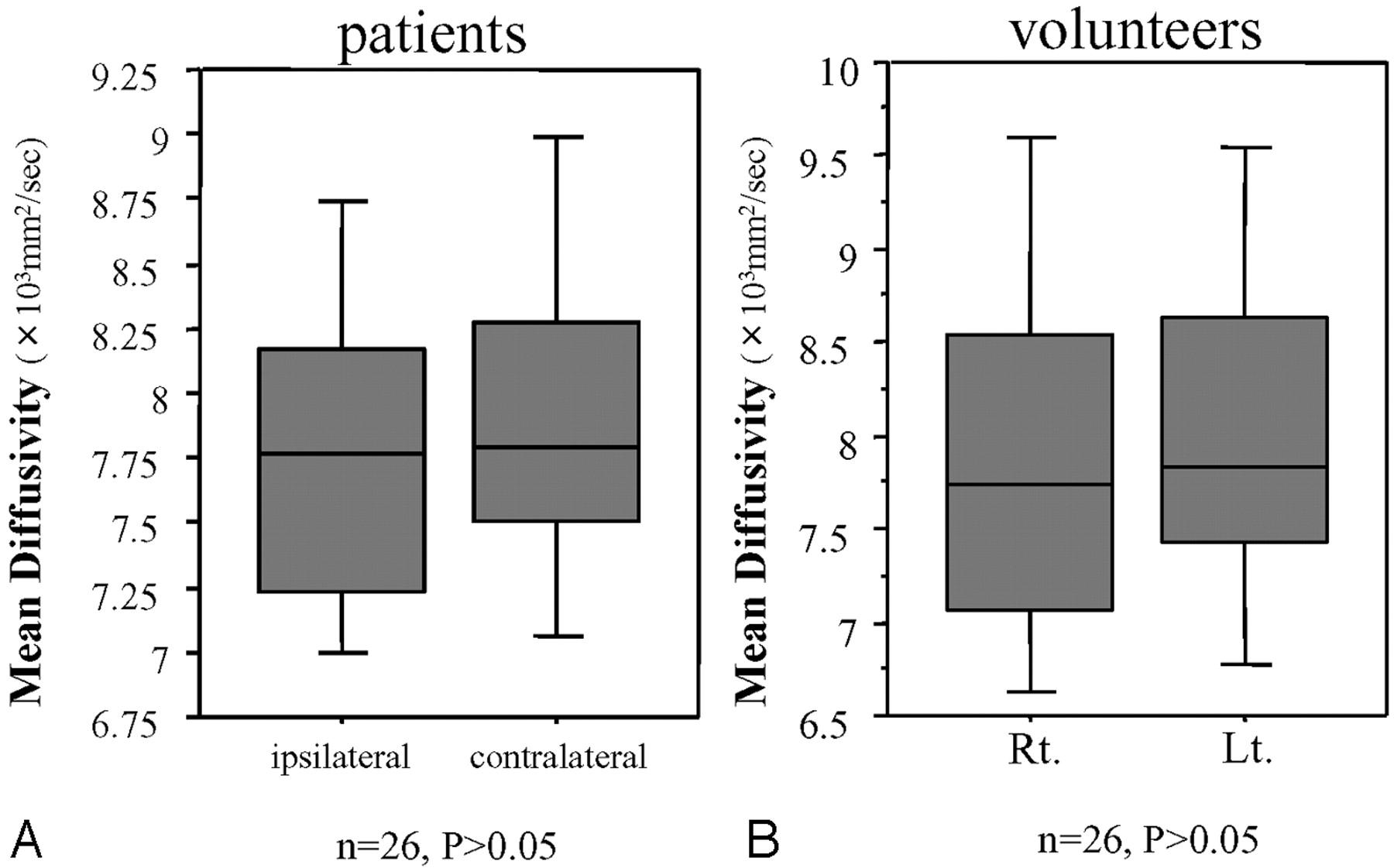
In healthy volunteers, there was no significant difference in FA values between bilateral pyramidal tracts (right versus left, 0.72 ± 0.05 versus 0.73 ± 0.03; P = .46). On the other hand, in patients with CSDH, the FA value of the pyramidal tract on the lesion side was significantly lower than that on the contralateral side (0.66 ± 0.07 versus 0.74 ± 0.05, P < .0001) (Fig. 2). With regard to the MD value, in patients and healthy volunteers, there was no significant difference in bilateral tracts (patients: 8.0 ± 0.8 10−4 mm2/s versus 8.1 ± 1.1 10−4 mm2/s, P > .05; volunteers: 7.9 ± 1.2 10−4 mm2/s versus 8.0 ± 1.1 10−4 mm2/s, P > .05) (Fig 3).

Region-of-interest analysis of FA values in the cerebral peduncle for lesion sides and contralateral sides. The Wilcoxon signed rank test was used for analysis of the differences. A, In patients with CSDH, FA values of the affected sides are significantly lower than those of intact sides (P < .0001). B, In healthy volunteers, there is no significant difference between bilateral sides (P > .5). Lt. indicates left; Rt, right.

Region-of-interest analysis of MD values in the cerebral peduncle for lesion sides and contralateral sides. The Wilcoxon signed rank test was used for analysis of the differences. A, In patients with CSDH, there is no significant difference in MD values between the affected sides and the contralateral sides (P > .5). B, In healthy volunteers, there is no significant difference between bilateral sides (P > .5). Lt. indicates left; Rt, right.
Linear regression analysis revealed that the preoperative FA ratio was significantly correlated to MMT (r2 = 0.32, P = .002) (Fig 4). The preoperative FA ratio was associated with the interval from the trauma and the midline shift determined on CT (interval from trauma, P = .0008; midline shift, P = .037). Age, hematoma thickness, and attenuation of the hematoma on CT were not associated with the FA ratio (P > .05) (Table 2). In 20 (87.0%) of 23 patients, the FA of the pyramidal tract on the lesion side after surgery increased significantly compared with that before the surgery (0.89 ± 0.08 versus 0.96 ± 0.08, P = .0004) (Fig 5). The other 3 patients (cases 14, 16, and 17) had no motor weakness before surgery.

The correlation between the initial FA ratio and motor weakness. Initial FA ratios are significantly correlated with motor weakness (R2 = 0.32, P = .002) by linear regression analysis. Preope. indicates preoperative.

The comparison FA ratios before and after burr-hole craniotomy in 23 patients with CSDH. FA ratios are significantly increased after surgery (Wilcoxon signed rank test, P = .0004). Pre-ope indicates preoperative; Post-ope, postoperative.
Relationship between clinical data and FA ratio
Discussion
CSDH generally occurs in the elderly, with a reported annual incidence of 5.3 patients treated per 10,0000 individuals.11 In 60%–80% of patients, a traumatic event is reported to precede the hemorrhage,2,12 but a mild traumatic event may go unrecognized. Traumatic subdural effusion is a result of arachnoid tearing caused by head injury or neurosurgery, and this fluid with or without blood in the subdural space facilitates the formation of a medial membrane. This medial membrane then forms internal capillaries or sinusoids. These fenestrated blood vessels allow plasma fluid leakage into and resultant enlargement of the subdural space. Bleeding then occurs repeatedly from capillaries, with the degeneration of the endothelium, and is accompanied by local hyperfibrinolysis, which is one of the causes of the growth of effusion into the CSDH. Among our patients, the common symptoms were gait disturbance, hemiparesis, headache, and dementia. Generally, in cases with symptomatic or expanding hematoma, a burr-hole craniotomy is performed. Following the surgical treatment, most patients with CSDH immediately and dramatically recover their premorbid function. Some previous reports have demonstrated that a reversible reduction of cerebral function can be caused by a decreased cerebral blood flow or vasogenic edema in the affected pyramidal tract; however, the detailed physiology has remained controversial.13–15
In patients with CSDH, our results showed significantly reduced FA in the affected descending pyramidal tract on DTI, correlated with the severity of the motor dysfunction. These findings coincide with those of secondary degeneration caused by stroke, tumor, trauma, and so forth, as demonstrated in previous reports.16–21 Moreover, our results showed significant improvement of the FA ratio with a rapid relief of motor weakness after hematoma removal. Recently, some reports have demonstrated cases with reversible loss of anisotropy in the white matter. Kim et al8 and Yamada et al22 reported that a decreased FA value on DTI did not necessarily represent direct damage to the tract but was more commonly noted to be a result of vasogenic edema and tract compression by the mass effect. Then, they believed that reversible loss of FA in cases of CSDH is incurred by the distortion of the pyramidal tract and vasogenic edema due to expansion of the hematoma.
In the factor analysis, the initial FA ratio was significantly associated with the interval from trauma and the midline shift (Table 2). Although there was no statistical significance, FA ratios tended to decrease in patients with mixed-attenuation hematoma on CT. These results indicated that a rapidly growing hematoma will invite severe distortion and vasogenic edema, which result in a decrease of the FA ratio. Finally, motor deficits are accompanied by decreased FA in the pyramidal tract. However, the thickness of the hematoma was not associated with the decreased FA ratio. It was believed that a thick hematoma sometimes causes only a tiny distortion and vasogenic edema in elderly patients with atrophic cerebral hemispheres.
There are certain limitations to this study. First, the patient population was small, and the power of statistical analysis was limited. In the present study, patients with bilateral CSDH were excluded because of the need to compare FA values of pyramidal tracts between affected and nonaffected sides. Second, all demonstrated FA values were analyzed in the cerebral peduncles, and data of FA values in other parts of the pyramidal tracts were not shown. In the present study, regions of interest were defined on the basis of an anatomic knowledge of the location of the pyramidal tract. Beforehand, we analyzed FA values not only in the cerebral peduncles but also in the corona radiata and internal capsule. The reproducibility of the obtained FA values in the cerebral peduncles was the most consistent among the 3 areas, so we chose the cerebral peduncles for analysis in this study. In the future, DTI will play an important role in clarifying the detailed physiology of CSDH. A much larger population of patients with CSDH must be subjected to DTI to accomplish this clarification.
Conclusion
Using DTI, we confirmed a reversibility of the declined FA in the distal pyramidal tract of patients with CSDH. The reversible loss of FA was considered to be incurred by the distortion of the pyramidal tract and vasogenic edema due to expansion of the hematoma.
References
- Received October 23, 2007.
- Accepted after revision December 23, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}