
Abstract
BACKGROUND AND PURPOSE: The intrasaccular flow disruptor, the Woven EndoBridge device, is increasingly used for the treatment of wide-neck intracranial aneurysms. Due to unfavorable anatomy, additional stent placement is sometimes required to avoid Woven EndoBridge protrusion into bifurcation branches. We report our experience with the Woven EndoBridge associated with stent placement for the treatment of complex intracranial aneurysms.
MATERIALS AND METHODS: Patients with aneurysms treated with the Woven EndoBridge Single-Layer plus stent placement were evaluated retrospectively with prospectively maintained data. The technical feasibility, procedural complications, aneurysm occlusion, and clinical outcome were studied.
RESULTS: Seventeen patients and aneurysms treated with the Woven EndoBridge plus stent placement were included. The mean aneurysm size was 7 ± 3.1 mm. Aneurysm locations were the following: MCA (10 patients), anterior communicating artery (3 patients), basilar tip (3 patients), and posterior communicating artery (1 patient). Two lesions were ruptured and treated in the acute phase. The Woven EndoBridge and stent placement were successfully delivered in all cases. There were no permanent/major complications. Among the 2 patients with SAH, minor and completely reversible in-stent thrombosis occurred during treatment. An asymptomatic occlusion of the angular artery with a distal nonbifurcation aneurysm was discovered during the angiographic follow-up. Long-term (10.4 months) angiographic complete (Raymond-Roy I) and near-complete (Raymond-Roy II) occlusion was obtained in 11 (69%) and 2 (12.5%) aneurysms, respectively. The mean sizes of aneurysms showing Raymond-Roy I/Raymond-Roy II and Raymond-Roy III occlusion were 5.5 ± 2.1 mm and 10 ± 1 mm, respectively (P = .003). The mean fluoroscopy time was 35 ± 14 minutes.
CONCLUSIONS: Aneurysm embolization with the Woven EndoBridge device associated with stent placement appears technically feasible and effective for the treatment of lesions with unfavorable anatomy. In our study, this strategy was relatively safe with a low rate of relevant procedure-related adverse events.
ABBREVIATIONS:
- AcomA
- anterior communicating artery
- PcomA
- posterior communicating artery
- RR
- Raymond-Roy
- SL
- Single-Layer
Despite the increased operator experience and the improvement of available devices, the endovascular treatment of wide-neck intracranial aneurysms, especially at bifurcation points, remains challenging. Accordingly, more complex endovascular techniques have been developed such as balloon-assisted coiling, stent-assisted coiling, and flow diversion.1,2 The intrasaccular flow disruptor, the Woven EndoBridge device (WEB; Sequent Medical, Aliso Viejo, California), is now a well-established option for the treatment of wide-neck bifurcation aneurysms.3⇓⇓–6 However, although the WEB treatment procedure is usually a single-step technique, additional stent placement can sometimes be required to prevent the protrusion of the device into the bifurcation arteries.7 To date, there are no series specifically evaluating treatment-related outcomes of the WEB associated with additional stent placement, to our knowledge. We present a retrospective series of 17 consecutive aneurysms treated with WEB plus stent placement at our institution, discussing the safety and efficacy of this treatment strategy.
Materials and Methods
Patient Selection
Our hospital institutional review board approved this retrospective study. The prospectively maintained data bases of WEB devices (from January 2014 to December 2018) at our institution were retrospectively reviewed by 2 and, in case of inconsistency, by 3 investigators independently to identify patients with intracranial aneurysms treated with the WEB and requiring additional stent placement to protect the vessel. We included aneurysms embolized with the WEB plus a stent in the same treatment session, excluding lesions in which stent placement was performed in a second treatment. Data collection included the following: demographics, aneurysm characteristics, clinical presentation, details of the treatment, follow-up imaging, and clinical outcome. Treatment strategy was decided by multidisciplinary consensus (vascular neurosurgeons, interventional neuroradiologists). The decision to treat with the WEB plus stent placement was made on the basis of the following situations: 1) planned stent placement: wide-neck lesions with branching vessels coming from the aneurysm for which treatment with adjunctive stent placement was planned beforehand because of the risk of WEB protrusion into the vessel; and 2) unplanned stent placement: slow flow or narrowing of the bifurcation vessel after WEB deployment due to the protrusion of the device into the artery.
Antiplatelet Therapy
For unruptured aneurysms, antiplatelet therapy included daily dual-antiplatelet medication with aspirin (Kardegic), 75 mg, and clopidogrel (Plavix), 75 mg, starting 5 days before treatment. The therapy was maintained for 3 months. In general, on the basis of the clinical and radiologic evaluations, the patients were switched to aspirin. The VerifyNow P2Y12 assay (Accumetrics, San Diego, California) was used to test the platelet inhibition: Both the P2Y12 and aspirin reaction units were tested. When stents and the WEB were used in patients with acutely ruptured aneurysms, an intravenous bolus of abciximab (0.125 mg/kg) was administered before stent deployment, and standard dual-antiplatelet therapy was started the day after. Concurrent with the procedure, in both unruptured and ruptured aneurysms, intravenous heparinization was performed (activated clotting time maintained above 250 seconds).
Description of Technique
All patients were treated under general anesthesia via a transfemoral approach. Access to the target aneurysm was obtained in a triaxial fashion. Through a long femoral sheath, a 6F guiding catheter was advanced into the carotid artery. Vessel and aneurysm features were analyzed via biplane and 3D rotational angiography. Size selection of the WEB was derived from the measurements of the aneurysm (width and height of the dome, width of the neck) based on a 3D rotational angiographic dataset. In general, the device was chosen adding 1 mm to the average width (to assure good wall apposition) and subtracting 1 mm from the average height of the aneurysm (to adjust for the longitudinal increase caused by the horizontal compression).8 An appropriate VIA Microcatheter (Sequent Medical) was placed inside the aneurysmal fundus followed by the deployment of the WEB under roadmap guidance.
The stent was selected on the basis of the diameter of the artery and was unsheathed under roadmap guidance through an appropriate microcatheter navigated beyond the aneurysm neck. Immediately postdeployment, VasoCT (Philips Healthcare, Best, the Netherlands) with diluted iodinated contrast medium was used to assess both the WEB and stent apposition.
Clinical and Imaging Assessment
Clinical evaluation was performed preoperatively, postprocedure, throughout the following days, and at discharge. The modified Rankin Scale was used for outcome assessment. Clinical follow-up evaluation was performed at 3, 6, 12, and 24 months. Usually, the degree of aneurysm occlusion was evaluated with MR angiography or digital subtraction angiography at 6 months, followed by long-term (12 and 24 months) DSA follow-up. The aneurysm occlusion rate was defined on the basis of the Raymond-Roy (RR) classification: complete occlusion (class I), residual neck (class II), and incomplete occlusion or residual aneurysm (class III).9
Statistical Analysis
All statistical analyses were performed with SPSS, Version 24 (IBM, Armonk, New York). Summary statistics are presented for all data available using means ± SDs for continuous variables and frequency tabulations for categoric variables.
Results
Baseline Population Characteristics
Population characteristics are summarized in On-line Table 1. In the 4-year period, 102 consecutive patients with unruptured and ruptured intracranial aneurysms were treated with the WEB. We extracted 17 patients treated with WEB plus stent placement (12 women, 5 men; mean age, 62 ± 8.9 years; range, 39–75 years). The pretreatment mRS score was 0 for 15 patients (88%), 1 for 1 patient (6%), and 4 for 1 patient (6%). Overall, 14 patients showed vascular risk factors: Two patients were hypertensive (14%), 5 patients were smokers (36%), and 7 patients were hypertensive and smokers (50%). Two patients were treated in the setting of acute SAH (patients 4 and 7).
Aneurysm Characteristics
The mean size of the aneurysms was 7 ± 3.1 mm (range, 3–11 mm). All the aneurysms arose from a bifurcation point or presented with a branching vessel coming from the neck. Only 1 patient (patient 13) presented with an aneurysm with a fusiform aspect arising along the wall of the angular artery (M3). The most common location was the MCA (10 patients), followed by the anterior communicating artery (AcomA) (3 patients), basilar tip (3 patients), and posterior communicating artery (PcomA) (1 patient). Fifteen aneurysms were unruptured (88%), whereas 2 (12%) lesions were acutely ruptured. Among the unruptured group, 1 aneurysm (6%) was previously coiled, and WEB plus stent placement was used because of recanalization after coiling (patient 17).
Treatment Characteristics and Technical Results
The Single-Layer (SL) WEB device was used in all the reported cases (On-line Table 2). Stent placement was performed with the Neuroform Atlas (Stryker Neurovascular, Kalamazoo, Michigan) in 14 cases (illustrative case in Fig 1) and with the LEO baby stent (Balt Extrusion, Montmorency, France) in 2 cases. One case of a large unruptured PcomA aneurysm was treated with the WEB plus the Pipeline Embolization Device (PED; Covidien, Irvine, California) (patient 6 and Fig 2). Among 10 patients (58%), stent and WEB were planned before the treatment. A single stent was used in all except 2 cases (patients 3 and 17 treated with Y-stent placement) (illustrative case in Fig 3). In all cases, the WEB and stent were successfully navigated to the target area and deployed inside the sac and across the aneurysm neck, respectively. The mean intervention time was 78 ± 19 minutes (range, 50–105 minutes). The mean fluoroscopy time was 35 ± 14 minutes (range, 17–70 minutes).

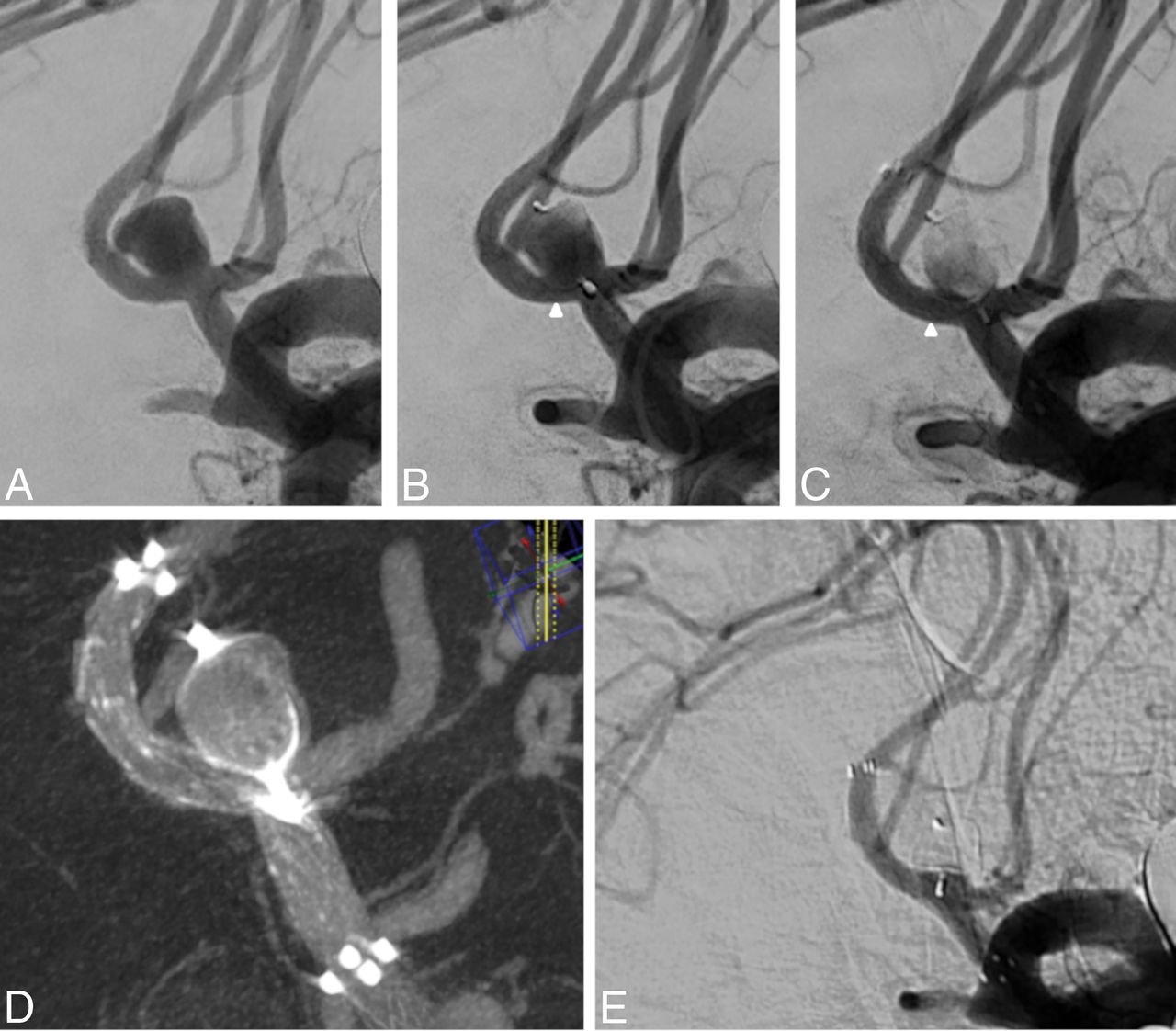
A, Patient 5 with a 6 × 4 mm unruptured AcomA aneurysm. B, A WEB-SL (7 × 3 mm) is opened inside the sac, with good aneurysm wall apposition and without impacting the branching vessels. However, after deployment, a protrusion occurred in the right A2 segment, leading to a stenosis (white arrowhead). C, A laser-cut Neuroform Atlas stent (3 × 20 mm) is then delivered to protect the caliber of the artery (white arrowhead). D, A final VasoCT confirms the satisfactory position and wall apposition of the stent and the WEB. E, Twelve-month DSA follow-up shows complete occlusion of the aneurysm.

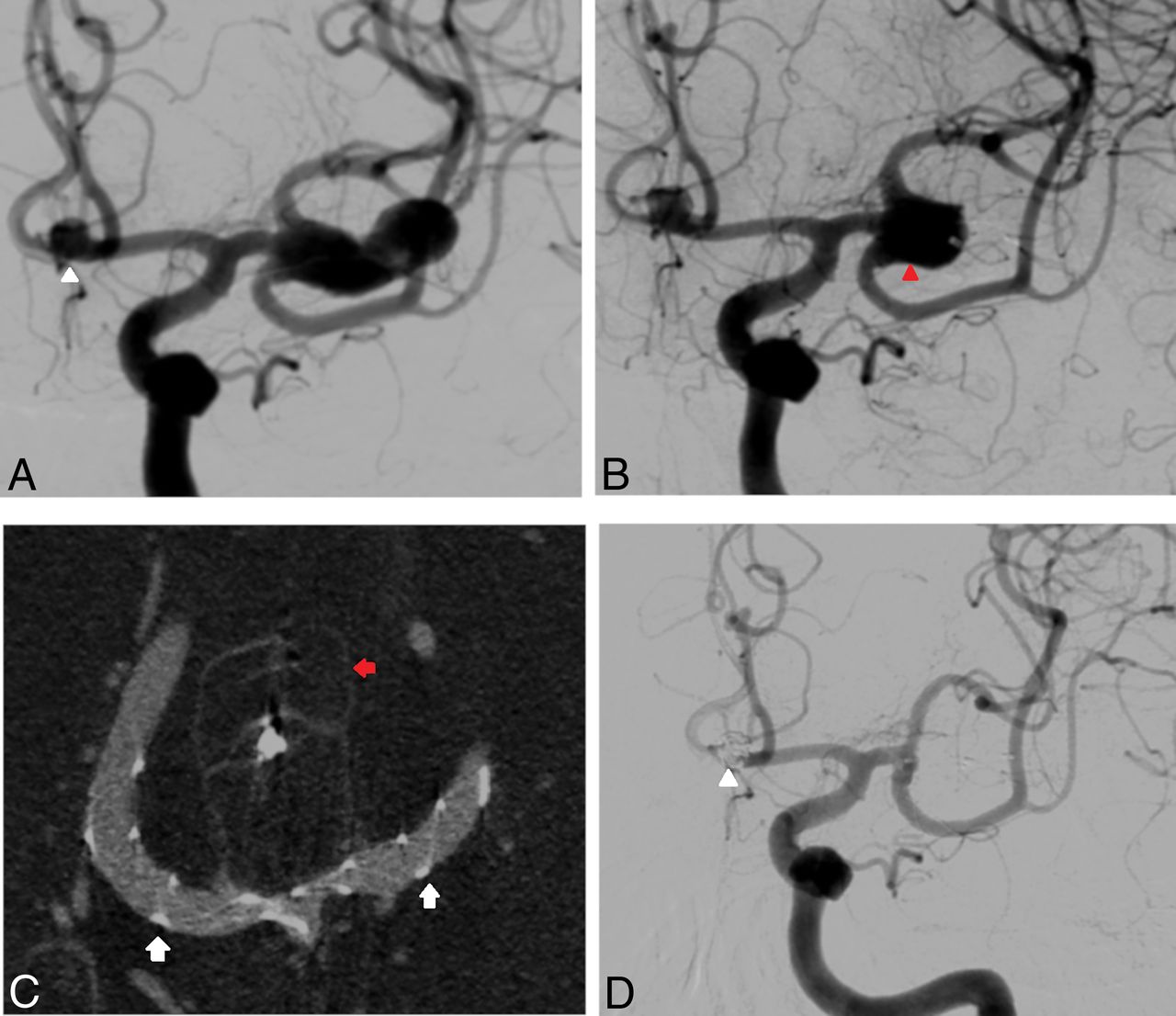
A, Right ICA angiography depicting a 9 × 10 mm PcomA unruptured aneurysm. A fetal variant of the PcomA arises from the aneurysm (red arrows). B, A WEB-SL (10 × 5 mm) was delivered inside the sac, intentionally undersized with respect to the origin of the fetal PcomA. Subsequently, a PED, 3.5 × 18 mm, was implanted from the right ICA to the right M1, covering the aneurysm neck, the PcomA, and the right A1. C, Flat panel CT reconstruction shows successful WEB and flow-diverter implantation and correct vessel wall apposition. D, Fifteen-month DSA follow-up shows complete occlusion of the aneurysm and the narrowing of the covered right A1 (white arrowheads).

A, Patient 3 with a left large (14 × 7 mm) unruptured aneurysm originating from the MCA bifurcation and another small unruptured aneurysm of the AcomA (white arrowhead). B, The MCA aneurysm, initially treated with a WEB-SL (9 × 6 mm), presents with a large recanalization (red arrowhead) due to WEB compaction. C, VasoCT shows the retreatment with a second WEB-SL (9 × 6 mm) associated with 2 Y-configurated LEO baby stents (2 × 18 mm) deployed from the M1 to the superior and inferior M2 branches (small white arrows). The first WEB appears compacted (small red arrow). D, Thirty-six-month DSA follow-up shows complete occlusion of the aneurysm. Both M2 branches are normal in caliber. The small AcomA aneurysm was coiled in another treatment session (white arrowhead).
Clinical Outcome and Procedure-Related Complications
Treatment-related complications and clinical outcomes are summarized in On-line Table 2. There were no permanent complications. Overall, 2 patients showed mild intraprocedural in-stent thrombosis completely reversible after abciximab injection (0.125 mg/kg). In these 2 cases, stent placement was performed in the setting of acute SAH: The bifurcation vessel presented slow flow due to a mild WEB protrusion, and the stent was placed to protect the branch (patients 4 and 7). During follow-up, patient 13, with a distal nonbifurcation MCA aneurysm, presented with a completely asymptomatic occlusion of the vessel after 12 months of DSA follow-up (Fig 4).

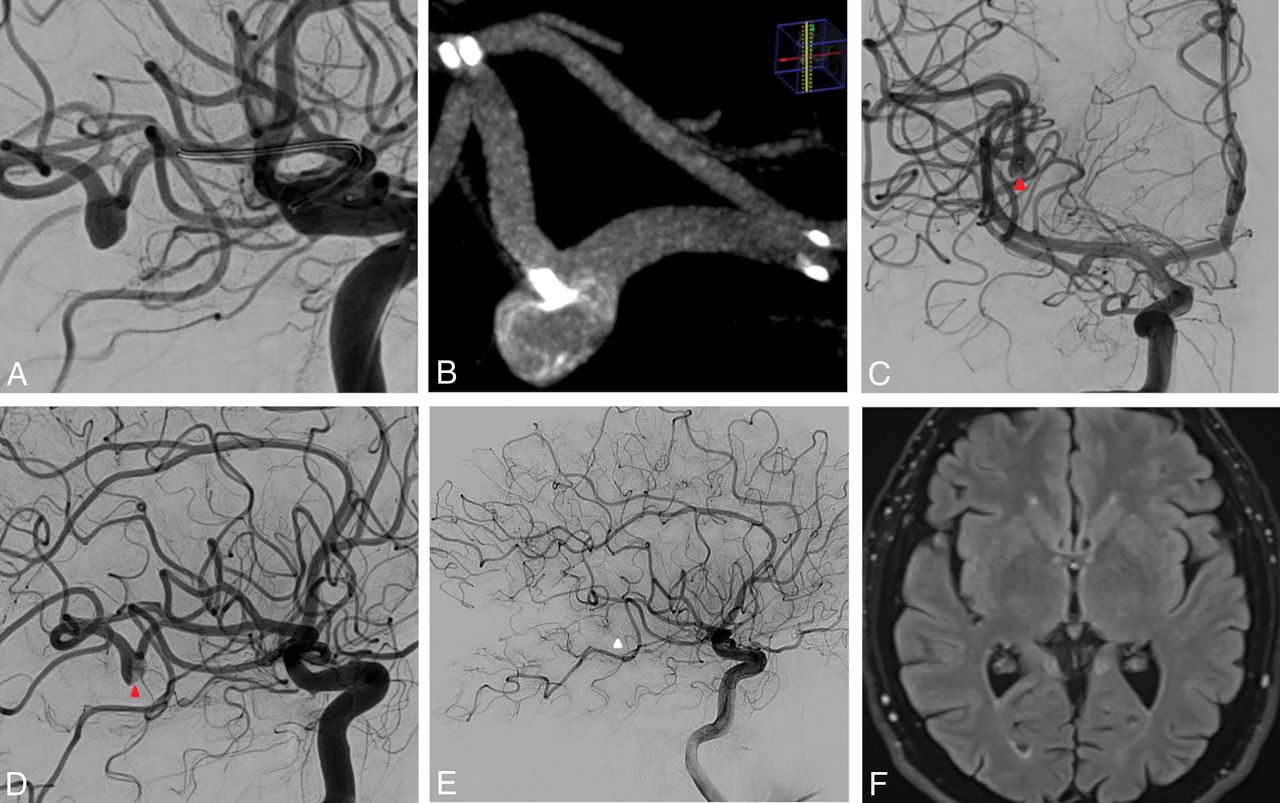
A, Patient 13 with a 5 × 4 mm unruptured nonbifurcation aneurysm arising from the wall of the distal portion of the angular artery (right MCA). B, VasoCT depicts the correct deployment of a WEB-SL (6 × 3 mm) into the sac associated with a Neuroform Atlas, 3 × 24 mm, delivered into the artery. Anteroposterior (C) and lateral (D) posttreatment angiograms show contrast agent stagnation into the aneurysm (red arrowhead). E, Twelve-month DSA follow-up (lateral view) shows the asymptomatic occlusion of the parent artery (white arrowhead). F, A FLAIR brain MR imaging sequence shows no associated ischemic lesions.
The mean fluoroscopy time among patients reporting intraprocedural ischemic events versus patients without intraprocedural complications was 51.5 ± 18.5 minutes versus 33 ± 3.1 minutes, respectively (P = .08), whereas the mean intervention time was 100 ± 0 minutes and 76 ± 18.5 minutes, respectively (P = .09). During long-term clinical follow-up (mean clinical follow-up, 11 months; range, 6–36 months), there were no modifications of the mRS related to the treatment. Overall, 14 patients presented with mRS 0, one patient presented with mRS 1, one patient (with a previous SAH from another aneurysm) presented with mRS 4, and 1 patient died due to the complications of the SAH.
Angiographic Outcome of Aneurysms
The mean radiologic follow-up was 10.4 months (range, 6–36 months) (On-line Table 2). Immediate complete occlusion (Raymond-Roy [RR] I) after treatment was achieved in 6 aneurysms (35%); 1 aneurysm (6%) showed a neck remnant (RR II), whereas 10 aneurysms (59%) were incompletely occluded (RR III). Sixteen patients were available for long-term angiographic follow-up. Overall, 11 (69%) aneurysms were completely occluded, 2 lesions presented with neck remnants (12.5%), and 3 aneurysms (18.5%) showed incomplete occlusion and were retreated with Y-stent-assisted coiling.
The mean sizes of aneurysms with occlusion RR I/RR II and RR III were 5.5 ± 2.1 mm (range, 3–9 mm) and 10 ± 1 mm (range, 9–11 mm), respectively (P = .003). Immediately after treatment, 90% (9 of 10) of aneurysms showing RR III occlusion presented with contrast agent stagnation inside the sac. Of them, 77% (7 of 9) progressed to RR I/II occlusion during follow-up. There were no cases of aneurysm rupture during long-term follow-up. Three cases of asymptomatic mild stent stenosis (<50%) were observed and were related to in-stent intimal hyperplasia. In case of mild stent stenosis, aspirin was usually prolonged until the next radiologic follow-up.
Discussion
The safety and efficacy of the WEB device for the treatment of wide-neck intracranial aneurysms, particularly for lesions challenging to treat with standard coiling, have been reported in several studies.5,6,10,11 However, treatment-related outcomes after intrasaccular flow-disruption with the WEB used with stents were not evaluated. We report the first series of a “stent-assisted WEB” used for the treatment of intracranial aneurysms in different locations.
Technical and Angiographic Outcomes
The WEB and the stent were successfully deployed inside the aneurysm and the artery in all cases, highlighting the feasibility of this technique. Consistent with the literature of WEB devices,5,10 initial complete/near-complete occlusion immediately after WEB and stent deployment was obtained in 41% of patients, whereas long-term adequate occlusion (RR I/RR II) was 81%. These results appear quite comparable with the angiographic outcome of other endovascular treatment modalities. In a meta-analysis of nearly 1900 aneurysms treated with stent-assisted coiling, the rates of immediate and long-term complete/near-complete occlusion were 54% and 73%, respectively.12 However, in our study, 3 aneurysms (18%) were incompletely occluded at follow-up and required retreatment with Y-stent-assisted coiling. Although the rate of retreatment was quite high, all of these were large aneurysms located at the basilar tip (On-line Tables 1 and 2). In a recent series of 79 endovascularly treated basilar tip aneurysms, the rate of incomplete occlusion was close to 40%, and large aneurysm size was reported as an independent risk factor for incomplete occlusion.13 Similarly, Abecassis et al14 reported a retreatment rate close to 40% among basilar tip aneurysms treated with endovascular techniques. Accordingly, in our experience, the stent-assisted WEB technique was associated with good angiographic results, except for large aneurysms of the basilar tip, where the bifurcation configuration and the hemodynamic forces may play an important role in the aneurysm recanalization.15
Among the published series of the WEB, the rate of treatment with the WEB and additional stent placement ranged between 5%6 and 18%.7,16 In general, the stents were implanted due to a suboptimal placement of the WEB inside the sac with a protrusion of the device inside the artery. Kabbasch et al,16 in a series of 114 intracranial aneurysms treated with the WEB, described 14% of cases requiring additional stent placement, reporting 69% adequate occlusion during follow-up.
In our series, as reported above, the decision to stent the artery was planned before or was made during treatment after deployment of the WEB. In the first situation, during the preoperative planning, the main morphologic factors indicating the need for additional stent placement were the presence of a wide neck and a vessel arising from the aneurysm sac. Thus, the possibility of WEB protrusion into the artery was considered not negligible, and stent placement was planned beforehand. An example is reported in Fig 4, in which a case of nonbranching 5 × 4 mm aneurysm arising from the wall of the angular artery is depicted. The strategy was to exclude the aneurysm with a WEB-SL (6 × 3 mm) and to protect the artery with a Neuroform Atlas (3 × 24 mm). Fig 2 shows another example of planned WEB plus stent placement. The WEB was intentionally undersized to avoid the coverage of the fetal PcomA coming from the aneurysm; accordingly, due to a large basal aneurysm remnant, a PED was deployed from the internal carotid artery to the M1 segment to cause a diversion of the flow from the residual aneurysm. In our opinion, given the undersized device, the risk of WEB compaction and aneurysm recanalization during follow-up was high; consequently, we decided to use a flow-diversion device in the same treatment session.
A third example is reported in Fig 3, depicting a large MCA bifurcation aneurysm recanalized after treatment with a WEB-SL. When we opened the first WEB, an immediate complete aneurysm exclusion was noticed, and no additional devices were used in the first session. However, likely due to the undersized WEB, the aneurysm was recanalized and the WEB was compacted at the midterm follow-up. A second WEB was deployed covering the aneurysm neck, while the M2 branches arising from the sac were protected with a Y-stent placement with 2 LEO baby stents. Complete aneurysm occlusion was achieved during follow-up.
On the other hand, when stent placement was not planned, the decision to stent the artery was because of the WEB protrusion into the bifurcation vessel. Fig 1 shows a wide-neck 6 × 4 mm AcomA aneurysm treated with a WEB-SL (7 × 3 mm). The WEB was protruding into the right A2, leading to a severe stenosis. Accordingly, a laser-cut stent was delivered to restore the caliber of the artery.
In general, larger aneurysms treated endovascularly are associated with lower rates of angiographic occlusion and a higher risk of recurrence.17 Accordingly, we found a significantly higher mean size among aneurysms incompletely occluded compared with those showing complete occlusion during follow-up (10 versus 5.5 mm, P = .003). This finding is line with a recent series investigating factors related to aneurysm occlusion after the WEB: The authors reported, in the multivariate analysis, that aneurysm size (OR = 1.2; 95% CI, 1.01–1.38; P = .034) was an independent morphologic risk factor for aneurysm remnants.16
Treatment-Related Complications
A recent large series and meta-analysis of the WEB for the treatment of intracranial aneurysms showed variable rates of treatment-related morbidity (between 2% and 10%).5,10 In our series, there were no permanent events or major neurologic complications. We describe 2 cases (patients 4 and 7) of intraprocedural complications after stent placement during acute SAH: A mild in-stent thrombosis was reported after stent deployment and was completely resolved after abciximab injection. During follow-up, only 1 patient (patient 13) had an asymptomatic parent vessel occlusion (angular artery) that was discovered during the angiographic long-term follow-up. It is likely that the artery was moderately stenosed by the WEB, and due to the collateral circulation, it became occluded without radiologic (the FLAIR findings were negative) and clinical sequalae (Fig 4).
Treatment with the WEB is, in general, a straightforward strategy, and this is mainly reflected by the brevity of the total fluoroscopic time reported in the literature. Fiorella et al3 in the WEB Intra-saccular Therapy Study (WEB-IT) reported a mean fluoroscopy time of 30 ± 15.7 minutes. Similarly, in a recent series of ruptured aneurysms treated with the WEB, the mean fluoroscopy time was 24 minutes (range, 8–40 minutes).18 It has been reported that longer intervention time (>120 minutes) is a risk factor associated with ischemic events after endovascular treatment of intracranial aneurysms.19 In our series, although some aneurysms required more complex treatment such as Y-stent placement plus a WEB, the mean intervention and fluoroscopy times were relatively low (78 and 35 minutes, respectively). Consistent with the literature, among patients reporting intraprocedural ischemic events, the mean fluoroscopy (51.5 versus 33 minutes) and intervention (100 versus 76 minutes) times were higher compared with those without complications.
Limitations of the Study
Our study has limitations intrinsic to single-center series. The number of patients is relatively small, though it is the first larger series investigating WEB-plus-stent placement. The data, though prospectively collected, were analyzed retrospectively. In addition, the imaging outcome was assessed by operators and not independently. There was a lack of standardization of radiologic follow-up.
Conclusions
Aneurysm embolization with WEB devices in association with stent placement appears both technically feasible and effective for the treatment of lesions with unfavorable anatomy, allowing high rates of long-term occlusion. In our study, this strategy was relatively safe with a low rate of relevant procedure-related adverse events.
Footnotes
Disclosures: Pierre-Henri Lefevre—UNRELATED: Payment for Development of Educational Presentations: Medtronic. Alain Bonafe—UNRELATED: Consultancy: Stryker Neurovascular, MicroVention. Vincent Costalat—UNRELATED: Consultancy: Medtronic, Stryker Neurovascular, Balt Extrusion, MicroVention; Grants/Grants Pending: Medtronic, Balt Extrusion*; Payment for Development of Educational Presentations: Medtronic, Balt Extrusion, Stryker Neurovascular. *Money paid to the institution.
REFERENCES
- Received January 3, 2019.
- Accepted after revision March 11, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Determinants of cerebral aneurysm occlusion after embolization with the WEB device: a single-institution series of 215 cases with angiographic follow-up
- Determinants of cerebral aneurysm occlusion after embolization with the WEB device: a single-institution series of 215 cases with angiographic follow-up
- Intracranial aneurysm treatment with WEB and adjunctive stent: preliminary evaluation in a single-center series
- Comparison of Woven EndoBridge device sizing with conventional measurements and virtual simulation using the Sim&Size software: a multicenter experience
- Virtual simulation with Sim&Size software for Pipeline Flex Embolization: evaluation of the technical and clinical impact
- Predicting Factors of Angiographic Aneurysm Occlusion after Treatment with the Woven EndoBridge Device: A Single-Center Experience with Midterm Follow-Up